

Pleural Metastasis as an Initial Presentation of Prostate Cancer: Case Report and Literature Review
- PMID: 40150008
- PMCID: PMC11940987
- DOI: 10.3390/diagnostics15060666
Pleural Metastasis as an Initial Presentation of Prostate Cancer: Case Report and Literature Review
Abstract
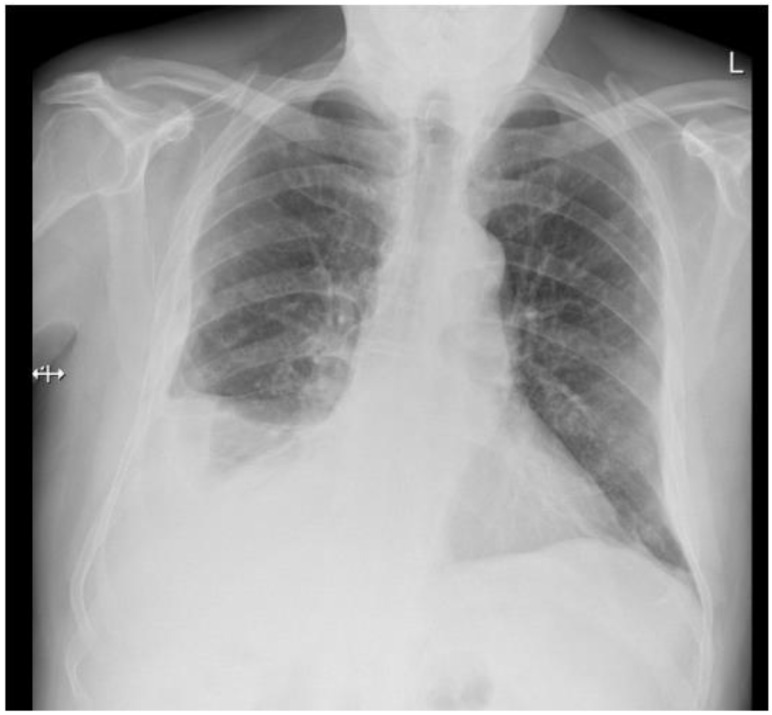
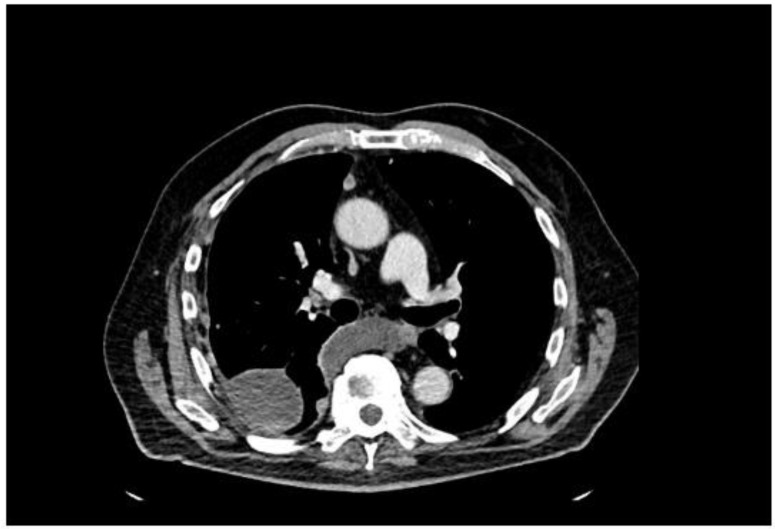
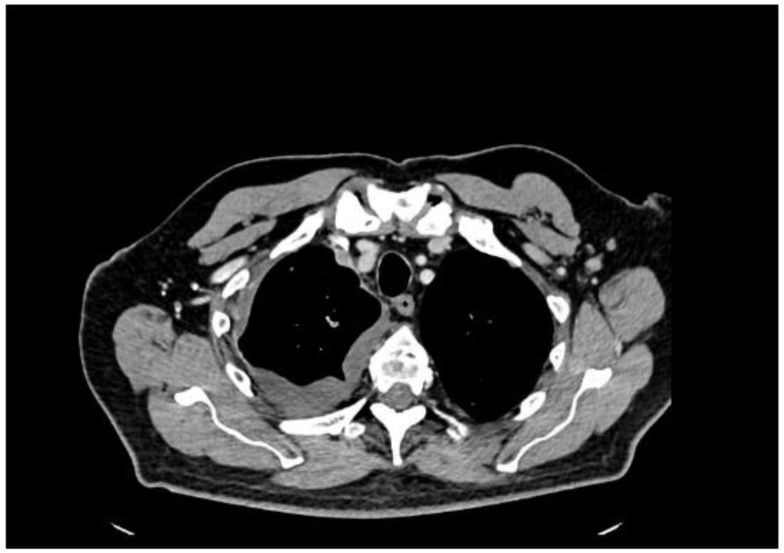
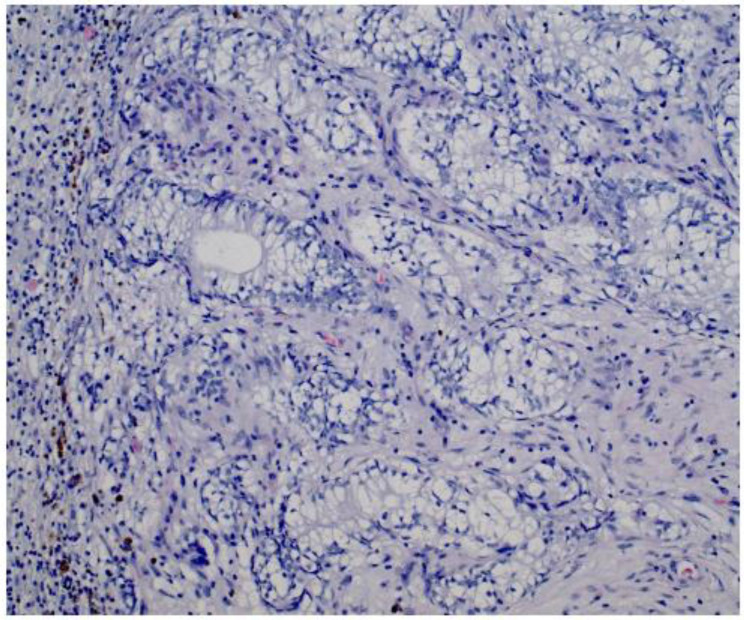
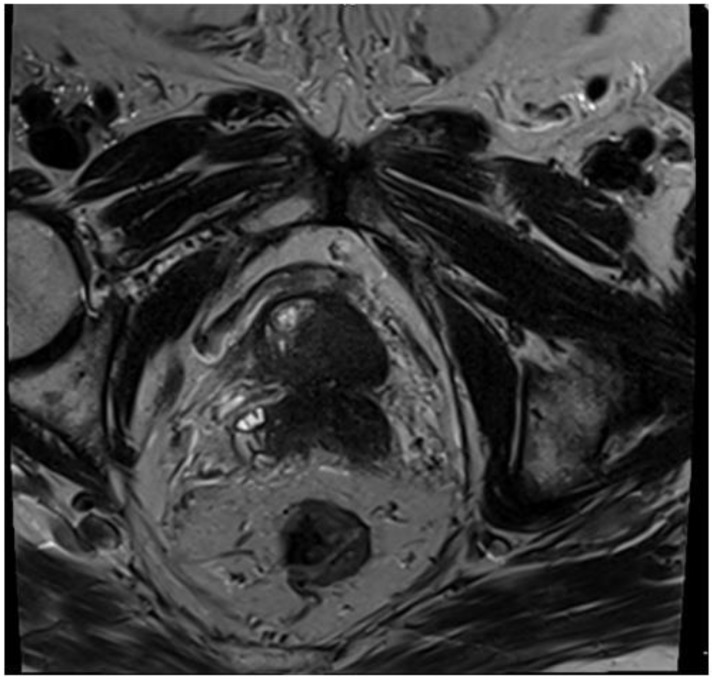
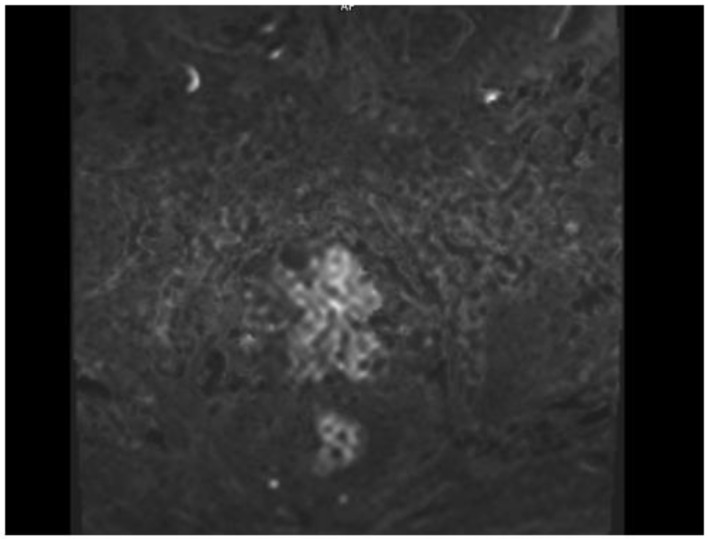
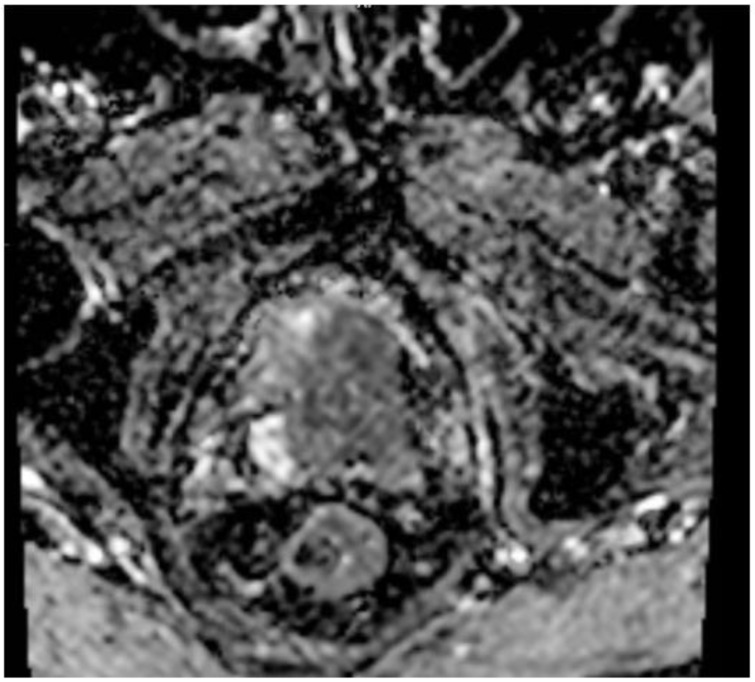
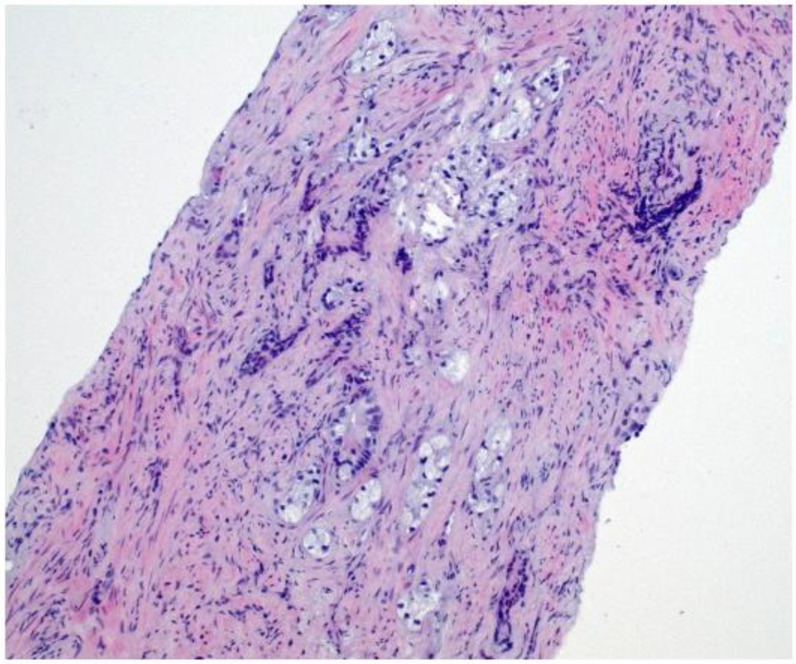
Background and Clinical Significance: Prostate cancer (PCa) is among the most commonly diagnosed malignancies in men worldwide. While bone and lymph nodes are the most frequent metastatic sites, prostate cancer cells have the potential to spread to virtually any organ, including the pleura, which is an exceedingly rare initial site of presentation that can mimic mesothelioma or primary lung cancer. Case Presentation: We describe a 77-year-old man who presented with exertional dyspnea and intermittent cough, initially suggesting a cardiopulmonary etiology. Imaging revealed multiple pleural nodules and an extensive right-sided pleural effusion. Despite a borderline serum prostate-specific antigen (PSA) level of 2.91 ng/mL, histopathology and immunohistochemistry of pleural biopsies confirmed metastatic prostate adenocarcinoma. Subsequent imaging identified a PIRADS 5 lesion in the prostate, and a biopsy confirmed ISUP Grade Group 5 disease (Gleason score 4 + 5 = 9). A bone scan showed no skeletal metastases, and a contrast-enhanced CT of the abdomen found no additional metastatic lesions. The patient was started on androgen deprivation therapy followed by abiraterone. This case underscores the diagnostic challenge posed by atypical metastatic presentations of prostate cancer. Low or moderately elevated PSA can obscure suspicion of prostate origin, especially with pleural-based lesions suggestive of mesothelioma. Immunohistochemical markers, including androgen receptors, AMACR, and Prostein, are critical for accurate diagnosis. Conclusions: Clinicians must maintain a high index of suspicion for prostate cancer in older men with unexplained pleural effusions, nodules, or masses, even with low-normal PSA levels. Early recognition and prompt treatment can improve outcomes, despite the rarity and aggressiveness of pleural metastases.
Keywords: low PSA; metastatic disease; pleural metastasis; prostate cancer.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ferlay J., Colombet M., Soerjomataram I., Parkin D.M., Piñeros M., Znaor A., Bray F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2020. Int. J. Cancer. 2021;149:778–789.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
