

Ruptured Intracranial Dermoid Cyst with Fat Dissemination: A Clinical Case Mimicking an Epidermoid Cyst and Review of the Literature
- PMID: 40150055
- PMCID: PMC11941323
- DOI: 10.3390/diagnostics15060712
Ruptured Intracranial Dermoid Cyst with Fat Dissemination: A Clinical Case Mimicking an Epidermoid Cyst and Review of the Literature
Abstract
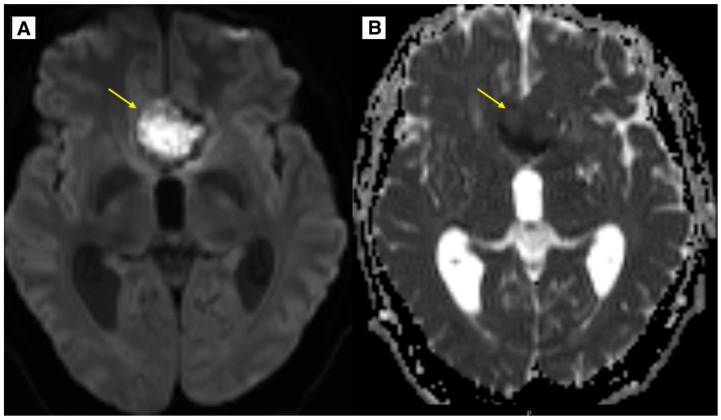
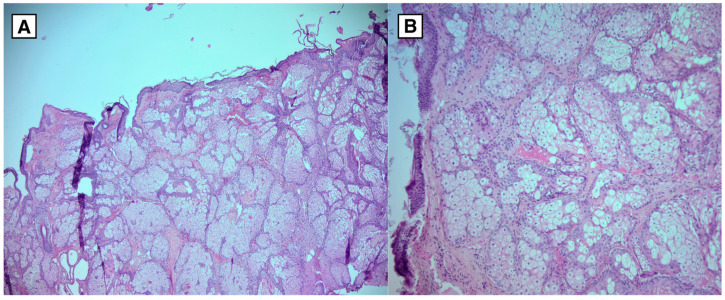
Background and Clinical Significance: Intracranial dermoid cysts (IDCs) are rare benign congenital intracranial lesions. In the case of IDC rupture, these lesions may manifest clinically. Cysts may be visualized on non-enhanced computed tomography (NECT) and magnetic resonance imaging (MRI), facilitating discussions between clinicians and radiologists to determine cyst content and potential dissemination in cases of rupture. This case report describes an IDC rupture presenting as fat-containing lesions in the subarachnoid space and ventricular system, resembling a subarachnoid hemorrhage on MRI. Case Presentation: A thirty-two-year-old Caucasian male patient was admitted to the hospital due to recurrent headaches and visual impairment that began at the age of thirty-one. MRI revealed a lesion radiologically consistent with a ruptured dermoid or epidermoid cyst in the anterior fossa with a mass effect on the optic nerve intracranial segments, the chiasma opticum, and proximal optic tracts. The patient underwent a successful neurosurgical resection of the lesion, and histopathological analysis confirmed the diagnosis of a dermoid cyst. The postoperative period was uneventful. MRI follow-up revealed residual tissue of the IDC without any volume increase. Multiple punctate fat-containing lesions were noted, similar to previous MRIs. The patient reported no complaints at discharge. Follow-up MRI imaging demonstrated no recurrence or progression of the dermoid cyst at 4 months, 1 year, and 2 years. Conclusions: IDC rupture is a rare event that may present clinically and appear as a blooming artifact on MRI, mimicking subarachnoid hemorrhage. Fat-containing lesions in the subarachnoid space and ventricular system can demonstrate findings indicative of an IDC rupture. MRI diffusion-weighted imaging (DWI) and decreased apparent diffusion coefficient (ADC) values may mimic an epidermoid cyst, a phenomenon rarely described in the literature, further complicating the diagnostic process.
Keywords: blooming artifact; epidermoid cyst; intracranial dermoid cyst rupture; intraventricular fat dissemination; subarachnoid fat dissemination.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Emmanuel S., Inban P., Akuma O., Nouman Aslam M., Talat F., Nizamani A., Chenna V.S.H., Romain E.M., Chu Carredo C.K., Khan A. An Atypical Case of Intracranial Dermoid Cyst in an Adult Female: A Case Report and Literature Review. Cureus. 2023;15:e39807. doi: 10.7759/cureus.39807. - DOI - PMC - PubMed
-
- Mouskou S., Stamati A., Sfakianos G., Malama A., Gavra M., Vartzelis G., Korona A., Mastrogianni S., Voudris K. Ruptured intracranial dermoid cyst in a child. Cause of atypical neurological symptoms. Interdiscip. Neurosurg. 2020;20:100482. doi: 10.1016/j.inat.2019.100482. - DOI
Publication types
LinkOut - more resources
Full Text Sources
