

Timely and Personalized Interventions and Vigilant Care in Neurodegenerative Conditions: The FIT4TeleNEURO Pragmatic Trial
- PMID: 40150532
- PMCID: PMC11942313
- DOI: 10.3390/healthcare13060682
Timely and Personalized Interventions and Vigilant Care in Neurodegenerative Conditions: The FIT4TeleNEURO Pragmatic Trial
Abstract
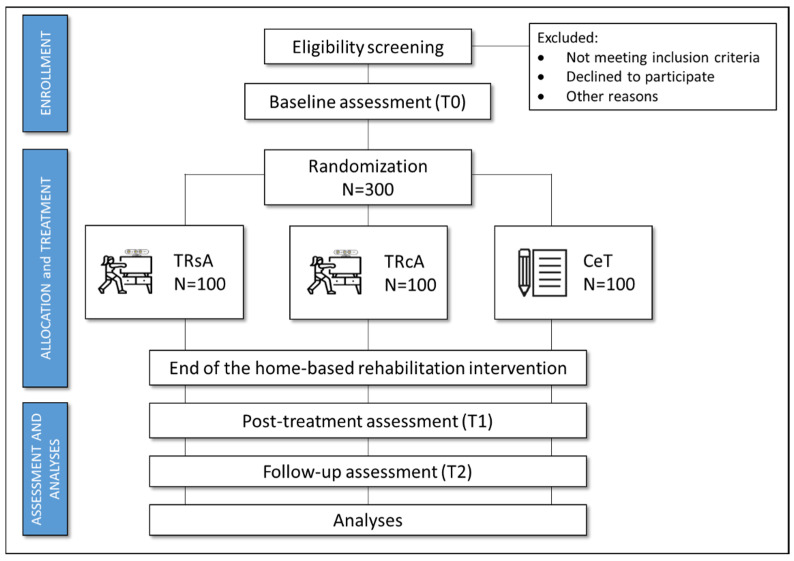
Parkinson's disease (PD) and multiple sclerosis (MS) are two chronic neurological diseases (CNDs) that have a high demand for early and continuous rehabilitation. However, accessing professional care remains a challenge, making it a key priority to identify sustainable solutions for ensuring early rehabilitation availability. Objective: The FIT4TeleNEURO pragmatic trial proposes to investigate, in real-life care settings, the superiority in terms of the effectiveness of early rehabilitation intervention with harmonized, mix-model telerehabilitation (TR) protocols (TR single approach, task-oriented-TRsA; TR combined approach, task-oriented and impairment-oriented-TRcA) compared to conventional management (control treatment, CeT) in people with PD and MS. Design, and Methods: This multicenter, randomized, three-treatment arm pragmatic trial will involve 300 patients with CNDs (PD, N = 150; MS, N = 150). Each participant will be randomized (1:1:1) to the experimental groups (20 sessions of TRsA or TRcA according to a mix-model-3 asynchronous + 1 synchronous session/week) or the control group (20 sessions of CeT). Primary and secondary outcome measures will be obtained at the baseline (T0), post-intervention (T1, 5 weeks after baseline), and follow-up (T2, 3 months after the end of the treatment). A multidimensional evaluation (cognitive, motor, and quality of life domains) will be conducted at each time point of assessment (T0; T1; T2). The primary outcome measures will be the assessment of change (T0 vs. T1 vs. T2) in static and dynamic balance, measured using the Mini-Balance Evaluation Systems Test. Usability and acceptability assessment will be also investigated. Expected Results: Implementing TR protocols will enable a more targeted and efficient response to the growing demand for rehabilitation in the early stages of CNDs. Both the TRsA and TRcA approaches are expected to be more effective than CeT, with the combined approach likely providing greater benefits in secondary outcome measures. Finally, the acceptability of the asynchronous modality could open the door to scalable solutions, such as digital therapeutics.
Keywords: Parkinson’s disease; chronic neurological diseases; digital medicine; multiple sclerosis; rehabilitation; telemedicine; telerehabilitation.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures



References
-
- Feigin V.L., Nichols E., Alam T., Bannick M.S., Beghi E., Blake N., Culpepper W.J., Dorsey E.R., Elbaz A., Ellenbogen R.G., et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:459–480. doi: 10.1016/S1474-4422(18)30499-X. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
