

Topohistology of dendritic cells and macrophages in the distal and proximal nodes along the lymph flow from the lung
- PMID: 40151162
- PMCID: PMC12265024
- DOI: 10.1111/joa.14251
Topohistology of dendritic cells and macrophages in the distal and proximal nodes along the lymph flow from the lung
Abstract
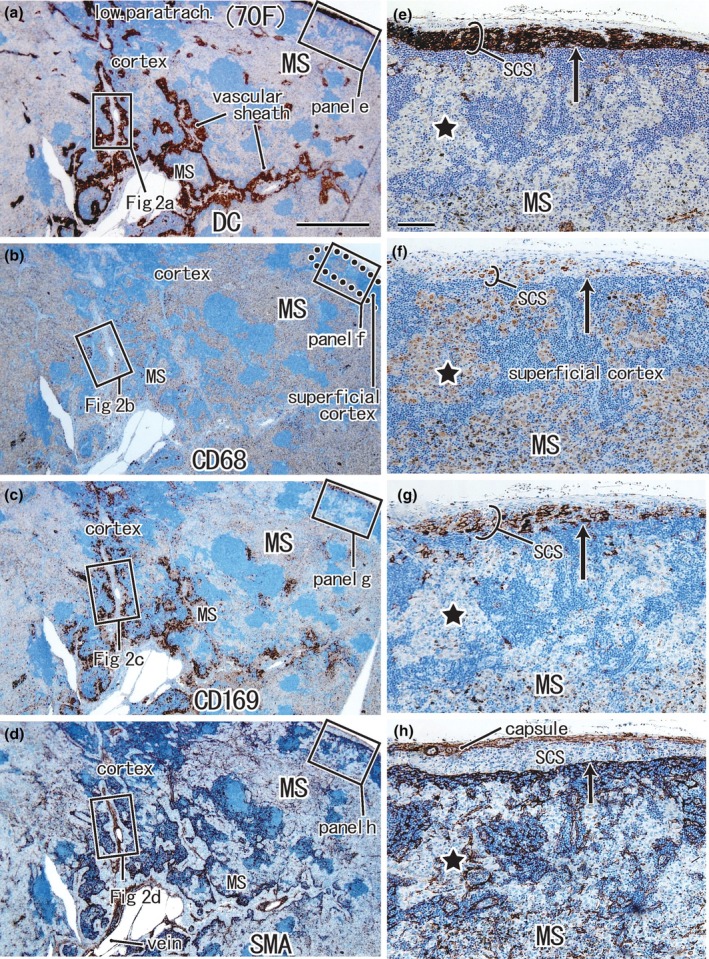
Nodal dendritic cells and CD169-positive macrophages cross-present cancer antigens earlier in the proximal nodes than in the distal nodes along the lymph flow from cancer. We examined topohistological differences between the proximal and distal nodes before the formation of metastasis. Immunohistochemical and morphometric analyses were performed to examine DC-SIGN-, CD68-, and CD169-positive cells in the subcarinal node (proximal) and paratracheal nodes (distal nodes) from 16 patients with lower-lobe lung cancer without metastasis (adenocarcinoma, 11; squamous, 5). Nodes at the same sites from 10 patients with upper-lobe cancer were used as controls. In all nodes, the medullary sinus was filled with CD68-positive and CD169-negative macrophages, most of which showed anthracosis. The proximal node carried a significantly smaller overlap between clusters of DC-SIGN-positive cells and CD169-positive cells relative to the distal node in lower-lobe cancer patients (p = 0.015). Irrespective of the cancer pathology, the tumor size was significantly correlated with the longer subcapsular clusters containing either DC-SIGN-positive cells or CD169-positive cells (p = 0.003, 0.043). A significantly small overlap between these clusters as well as the missing paracortical sinuses was evident in the negative control node outside the lymph flow (p = 0.006). Since DC-SIGN-positive cells and CD169-positive cells, especially composite cells in the overlapped cluster, are likely to be derived from monocytes, larger tumors appeared to accelerate the migration into the subcapsular sinus. In contrast to the suggested active status of the distal node, the proximal node appeared to have already been suppressed. This downregulation reached the level in the negative control node.
Keywords: CD169‐positive macrophages; anti‐cancer immunity; dendritic cells; lung regional node; morphometry; preconditioning along lymph flow; tumor size.
© 2025 The Author(s). Journal of Anatomy published by John Wiley & Sons Ltd on behalf of Anatomical Society.
Conflict of interest statement
The authors declare no conflicts of interest in association with the present study.
Figures





References
-
- Aokage, K. , Yoshida, J. , Ishii, G. , Hishida, T. , Nishimura, M. & Nagai, K. (2010) Subcarinal lymph node in upper lobe non‐small cell lung cancer patients: is selective lymph node dissection valid? Lung Cancer, 70, 163–167. - PubMed
-
- Asamura, H. , Nakayama, H. , Kondo, H. , Tsuchiya, R. & Naruke, T. (1999) Lobe‐specific extent of systematic lymph node dissection for non‐small cell lung carcinomas according to a retrospective study of metastasis and prognosis. The Journal of Thoracic and Cardiovascular Surgery, 117, 1102–1111. - PubMed
-
- Botella‐Estrada, R. , Dasi, F. , Ramos, D. , Nagore, E. , Herrero, M. , Gimenez, J. et al. (2005) Cytokine expression and dendritic cell density in melanoma sentinel node. Melanoma Research, 15, 99–106. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
