

Geriatric Vulnerabilities Among Adults With Heart Failure With Preserved Ejection Fraction: A Cross-Continent Evaluation
- PMID: 40155186
- PMCID: PMC11994044
- DOI: 10.1016/j.jacadv.2025.101602
Geriatric Vulnerabilities Among Adults With Heart Failure With Preserved Ejection Fraction: A Cross-Continent Evaluation
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) disproportionately affects older adults.
Objectives: This study aimed to elucidate the prevalence and prognostic implications of geriatric vulnerabilities across multiple health domains in HFpEF.
Methods: We examined consecutive patients with HFpEF enrolled from the Weill Cornell Medicine (WCM) and the OPTIMISE HFpEF Programs. The primary exposure was the following: multimorbidity, polypharmacy, cognitive impairment, depressive symptoms, frailty, and limited mobility. The primary outcome was a 1-year composite of all-cause hospitalization and mortality. We conducted Cox proportional hazard models to examine associations of the primary outcome with each geriatric vulnerability and the number of impaired domains, adjusting for race and the Meta-Analysis Global Group in Chronic Heart Failure risk score.
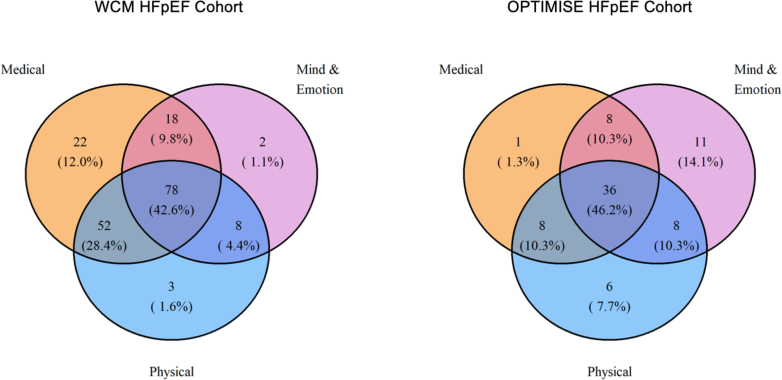
Results: The WCM cohort included 188 patients with a median age of 76.3 years, the majority of which were NYHA functional class III HF (52.1%); the OPTIMISE cohort included 93 patients with a median age of 79.6 years, the majority of which were NYHA functional class II HF (62.0%). Nearly half of each cohort (42.6% WCM, 46.2% OPTIMISE) had geriatric vulnerabilities spanning all 3 health domains. In fully adjusted models, frailty (WCM: HR: 2.89, 95% CI: 1.65-5.09; OPTIMISE: HR: 2.89, 95% CI: 1.65-5.09) and an increasing number of impaired domains were associated with the primary outcome: with 3 impaired domains conferring a near 4-fold increase in risk (WCM: HR: 3.97, 95% CI: 1.49-10.5, P = 0.007]; OPTIMISE: HR: 3.74, 95% CI: 1.26-11.10, P = 0.017]).
Conclusions: Geriatric vulnerabilities across multiple health domains commonly co-occur in adults with HFpEF and are associated with a worse prognosis.
Keywords: deprescribing; depression; frailty; geriatrics; heart failure; polypharmacy.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures Dr Goyal has received funding from National Institutes of Health grants K76AG064428, R21AG077092, and R01AG085420. Dr Turchioe has received funding from National Institutes of Health grants R00NR019124. Dr Creber has received funding from National Institutes of Health grants R01HL161458, R01NS123639, and R01HL152021. Dr Deaton has received funding from the National Institute for Health Research (NIHR) School for Primary Care Research, Addenbrooke’s Charitable Trust, Cambridge British Heart Foundation Centre of Research Excellence, and the NIHR Cambridge Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIH, NIHR, the NHS, or the Department of Health and Social Care. Dr Goyal has received consulting fees from Agepha Pharma, Akros Pharma, Axon therapies, Bayer HealthCare Pharmaceuticals, and Sensorum Health. Dr Turchioe has received fees from Boston Scientific and Iris OB health. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
