

Bone defects in knee revision arthroplasty-a therapy-oriented classification
- PMID: 40156618
- PMCID: PMC11954694
- DOI: 10.1007/s00402-025-05759-2
Bone defects in knee revision arthroplasty-a therapy-oriented classification
Abstract
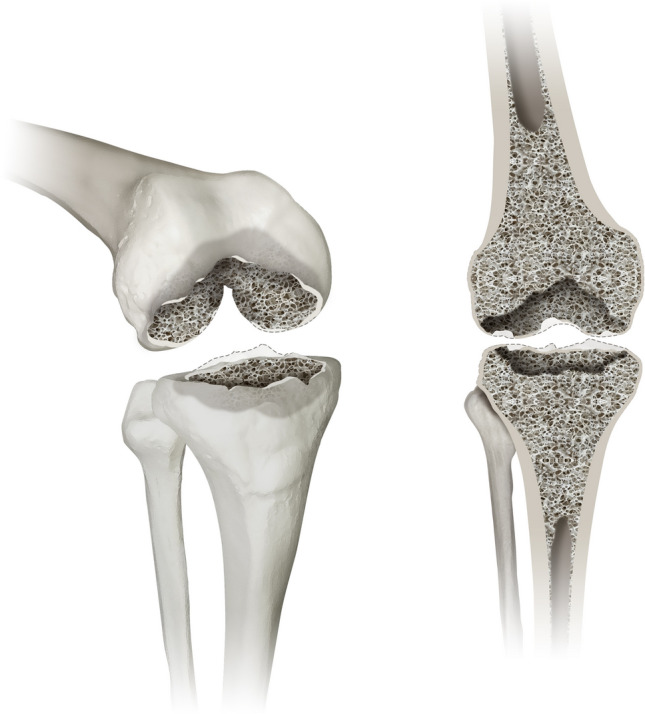
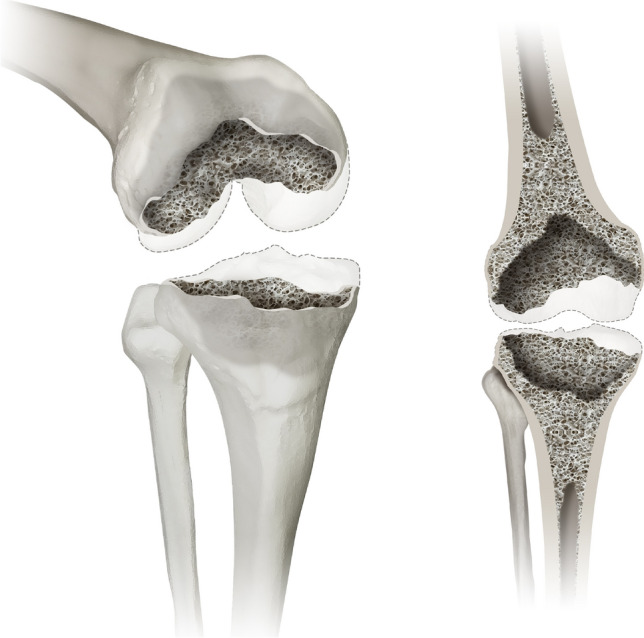
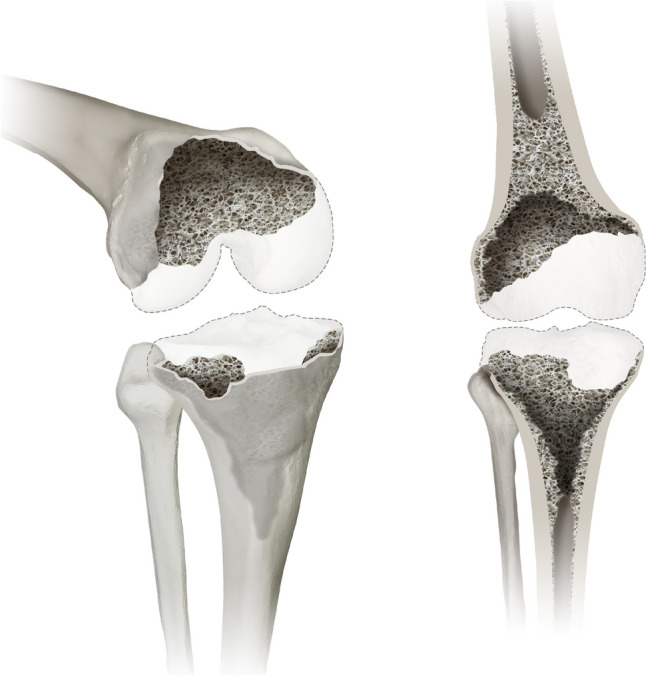
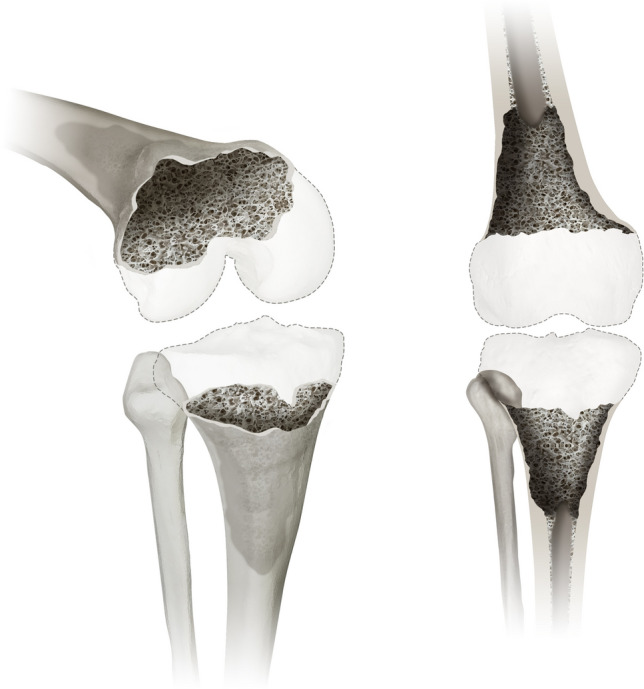
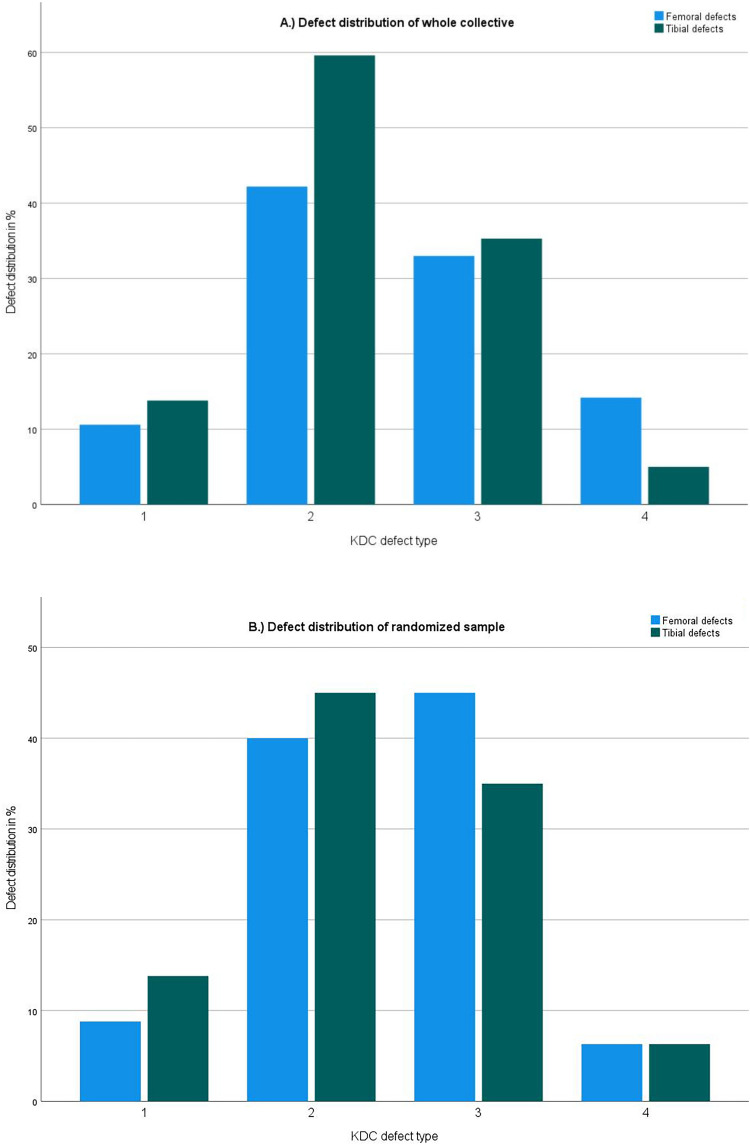
Introduction: The complex field of revision knee arthroplasty displays a lack of standardized, intuitive pre- and intraoperative assessment of bone defects. In clinical practice revision surgeries are a common sight presenting with increasingly complex cases of bone loss and ligamentary dysfunction. To address these issues the Knee Defect Classification (KDC) is introduced to offer a reliable, reproducible and an intuitive classification system with a clear therapeutic guideline.
Materials and methods: Reliability was evaluated through comparison between intraoperative findings and preoperative gradings of 218 patients. To account for reproducibility inter- and intra-rater agreement was assessed.
Results: The mean agreement between intraoperative and radiographic grading of femoral and tibial defects was evaluated with a Cohens kappa of 0.79, representing a good agreement. For interrater reliability a mean Fleiss kappa of 0.71 could be evaluated for femoral and tibial defects falling into the good agreement range. In the subgroup analysis femoral defects presented with a Fleiss kappa of 0.652 ± 0.026 (good agreement), while tibial defects presented with a Fleiss kappa of 0.768 ± 0.024 (good agreement). For intrarater reliability a mean Cohens kappa was evaluated at 0.78 indicating good agreement.
Conclusion: The KDC is a reliable and reproducible classification system. Through its structured design it facilitates intuitive use and allows for consistent preoperative planning and intraoperative guidance. A therapeutic algorithm is provided based on a review of the literature in combination with expert opinion.
Keywords: AORI; Constrainment; Defect classification; Knee revision arthroplasty; Ligamentary instability; Reliability; Reproducability.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: All authors declare that they have no conflict of interest. The authors did not receive support from any organization for the submitted work. Ethical approval and informed consent: All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. All data obtained is part of in-house quality assessment in accordance with National Register procedures. Additional approval for this study was obtained from the institutional review board of our hospital.
Figures



Similar articles
-
Femoral defects in revision hip arthroplasty: a therapy-oriented classification.Arch Orthop Trauma Surg. 2023 Mar;143(3):1163-1174. doi: 10.1007/s00402-021-04201-7. Epub 2021 Oct 12. Arch Orthop Trauma Surg. 2023. PMID: 34636979 Free PMC article.
-
Tibial bone defect prediction based on preoperative artefact-reduced CT imaging is superior to standard radiograph assessment.Knee Surg Sports Traumatol Arthrosc. 2023 Nov;31(11):4842-4850. doi: 10.1007/s00167-023-07527-4. Epub 2023 Aug 10. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37558747 Free PMC article.
-
A comparison between 3D printed models and standard 2D planning in the use of metal block augments in revision knee arthroplasty.Jt Dis Relat Surg. 2024 Aug 14;35(3):473-482. doi: 10.52312/jdrs.2024.1591. Epub 2024 Aug 14. Jt Dis Relat Surg. 2024. PMID: 39189555 Free PMC article.
-
Results of revision total knee arthroplasty in the face of significant bone deficiency.Orthop Clin North Am. 1998 Apr;29(2):361-71. doi: 10.1016/s0030-5898(05)70335-7. Orthop Clin North Am. 1998. PMID: 9553582 Review.
-
Techniques for filling tibiofemoral bone defects during revision total knee arthroplasty.Orthop Traumatol Surg Res. 2021 Feb;107(1S):102776. doi: 10.1016/j.otsr.2020.102776. Epub 2020 Dec 13. Orthop Traumatol Surg Res. 2021. PMID: 33321231 Review.
References
-
- Lübbeke A, Silman AJ, Barea C, Prieto-Alhambra D, Carr AJ (2018) Mapping existing hip and knee replacement registries in Europe. J Health Pol 122:548–557 - PubMed
-
- Charette RS, Sloan M, DeAngelis RD, Lee GC (2019) Higher rate of early revision following primary total knee arthroplasty in patients under age 55: a cautionary tale. J Arthroplasty 34(12):2918–2924 - PubMed
-
- Tarazi JM, Chen Z, Scuderi GR, Mont MA (2021) The epidemiology of revision total knee arthroplasty. J Knee Surg 34(13):1396–1401. 10.1055/s-0041-1735282 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
