

Drive-the-doctor paradigm in acute ischaemic stroke for improving regional stroke care networks: a cost-effectiveness analysis
- PMID: 40157729
- PMCID: PMC11956349
- DOI: 10.1136/bmjopen-2024-091413
Drive-the-doctor paradigm in acute ischaemic stroke for improving regional stroke care networks: a cost-effectiveness analysis
Abstract
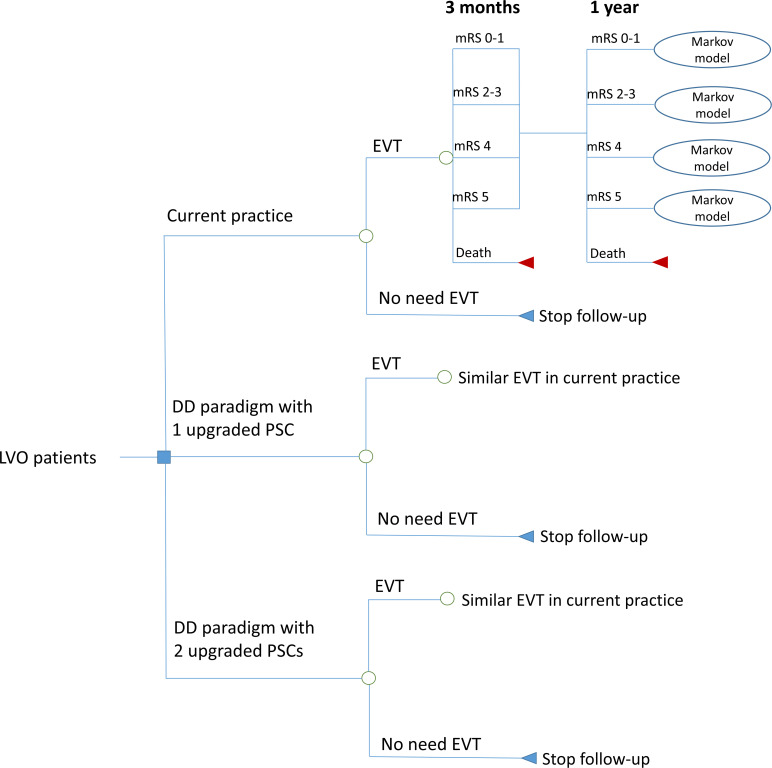
Background and objective: In a drive-the-doctor (DD) paradigm, an interventionalist travels from a comprehensive stroke centre (CSC) to primary stroke centres (PSCs) to perform endovascular thrombectomy (EVT) for acute ischaemic stroke due to large vessel occlusion (LVO). The DD paradigm may reduce time delays from onset to recanalisation. This study aimed to analyse the cost-effectiveness of the DD paradigm versus a drip-and-ship (DS) paradigm, where LVO patients are transferred from PSCs to a CSC for EVT in the northern Netherlands.
Design: Economic evaluation was performed using a simulation model combined with a decision tree and a Markov model.
Setting: Stroke centres in the northern Netherlands.
Participants: A hypothetical cohort of 100 000 LVO patients with an average age of 70 years.
Interventions: Two strategies were tested, including the DD paradigm with one upgraded PSC and the DD paradigm with two upgraded PSCs.
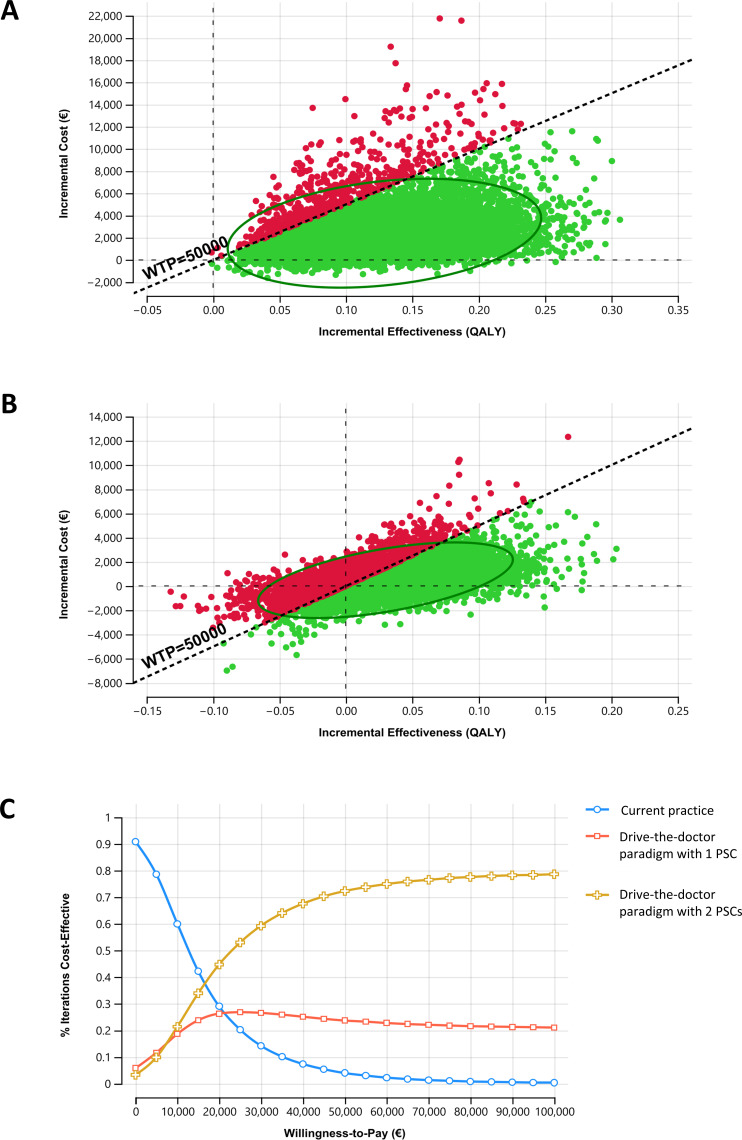
Main outcome measures: Total costs and quality-adjusted life years (QALYs) were measured over a 15-year time horizon from a Dutch healthcare provider perspective. An incremental cost-effectiveness ratio (ICER) of €50 000 was used as a willingness-to-pay threshold. One-way sensitivity, probabilistic sensitivity and scenario analyses (interventionalist transportation by car, ambulance and helicopter) were conducted to examine parameter uncertainty.
Results: The DD paradigm using car as a transport modality and two PSCs was the optimal strategy, resulting in the lowest ICER. This strategy provided an additional 0.13 QALYs at incremental costs of €2367, yielding an ICER of €18 306 compared with current practice. The DD paradigm with two PSCs reduced ICERs compared with the scenario with one PSC when varying transportation modalities (car, ambulance and helicopter). Probabilistic sensitivity analyses showed that the DD paradigm with two PSCs using car was preferred in 72% of 10 000 Monte Carlo simulations.
Conclusions: The DD paradigm appeared cost-effective for LVO patients and may be considered a promising evolution for a regional stroke network.
Keywords: HEALTH ECONOMICS; Organisation of health services; Stroke.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: EB reports funding from the Netherlands Heart Foundation and a Public Private Partnership allowance from Health Holland, ZonMw and NOW. EB serves at ZonMw committee as a (vice-) chairman, at ZuidOost Zorg and 113 Suicide Prevention as a member advisory board. MU has received research grants from ZonMw and Dutch Heart Foundation. DJVDZ is a member of the supervisory board Radiotherapeutisch Instituut Friesland.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical