

Temporal trends in hospitalisations for venous thromboembolic events in England: a population-level analysis
- PMID: 40157730
- PMCID: PMC11956333
- DOI: 10.1136/bmjopen-2024-090301
Temporal trends in hospitalisations for venous thromboembolic events in England: a population-level analysis
Abstract
Objectives: To describe temporal trends in hospitalisation episodes for venous thromboembolic events (VTEs) in England, and compare hospitalisation rates for pulmonary emboli (PEs) and deep vein thrombosis (DVT).
Methods: Retrospective observational study.
Setting: Secondary care in England, UK, between April 1998 and March 2022.
Participants: Individuals with hospitalisations for VTE recorded in the NHS Digital Hospital Episode Statistics dataset.
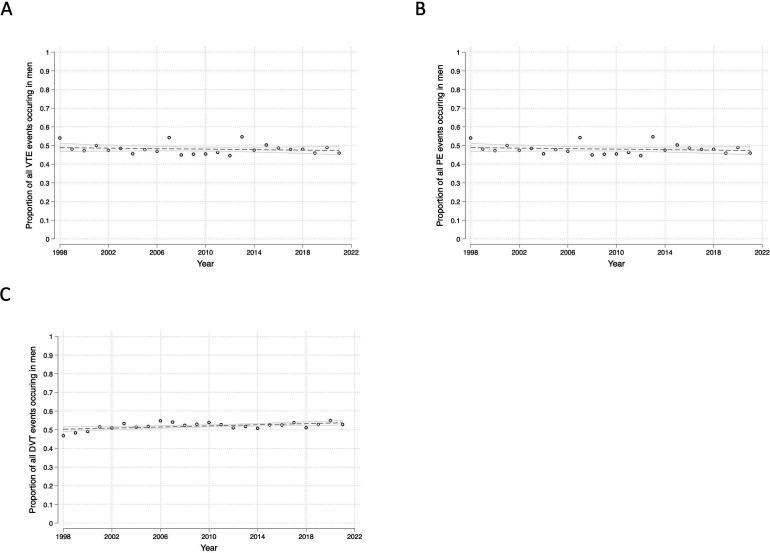
Primary and secondary outcomes: The primary outcome was temporal trends in hospitalisation episodes for PE, DVT and VTE overall between 1 April 1998 and 31 March 2022. Secondary outcomes included the proportion of all-cause hospital admissions that were due to VTE; the proportion of all VTE hospitalisations that were recorded as primary admission diagnoses; the male/female split in hospitalisation episodes for VTE; and temporal changes in hospitalisation rates by age.
Results: Between 1998 and 2022, hospitalisations for VTE increased by 62.6%, from 109.5 to 178.1 per 100 000 population. This was driven by a 202% increase in hospitalisations for PE (from 40.4 to 122.2 per 100 000 population). In contrast, hospitalisations for DVT decreased by 19.1% over this period (from 69.1 to 55.9 per 100 000 population). Overall, VTE remained stable as a proportion of all-cause hospital admissions between 1998/1999 and 2019/2020 (0.45% and 0.43%, respectively), before increasing after the onset of the COVID-19 pandemic in England (0.59% in 2020/2021 and 0.51% in 2021/2022).
Conclusion: Hospitalisations for VTE increased markedly in England between 1998 and 2022, driven by large increases in hospitalisations for PE. In contrast, hospitalisations for DVT decreased overall, which may reflect the success of primary care DVT management pathways. Our findings suggest that preventative measures are needed to reduce the incidence of hospitalisations for PE.
Keywords: COVID-19; EPIDEMIOLOGY; PUBLIC HEALTH; Primary Health Care; RHEUMATOLOGY; Thromboembolism.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: JBG has received honoraria from Abbvie, Biovitrum, BMS, Celgene, Chugai, Galapagos, Gilead, Janssen, Lilly, Novartis, Pfizer, Roche, Sanofi, Sobi and UCB. MDR has received honoraria from AbbVie, Lilly, Galapagos, Menarini and Viforpharma, advisory board fees from Biogen, and support for attending educational meetings from Lilly, Pfizer, Janssen and UCB. No other authors declared any conflicts of interest.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous