

Systematic review and meta-analysis of intravenous iron therapy for patients with heart failure and iron deficiency
- PMID: 40159279
- PMCID: PMC12353798
- DOI: 10.1038/s41591-025-03671-1
Systematic review and meta-analysis of intravenous iron therapy for patients with heart failure and iron deficiency
Abstract
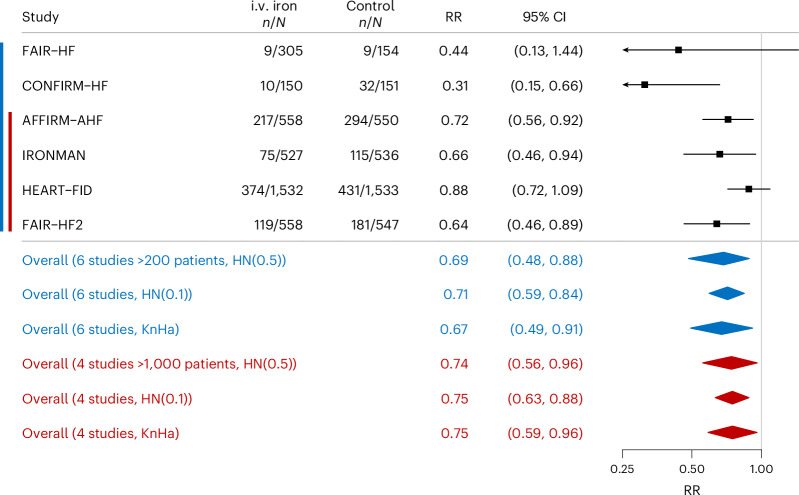
Uncertainty remains about the effect of intravenous (i.v.) iron on outcomes for heart failure (HF) with iron deficiency. In the present study, we summarize the efficacy and safety of i.v. iron from six trials (FAIR-HF, CONFIRM-HF, AFFIRM-AHF, IRONMAN, HEART-FID and FAIR-HF2), including 7,175 patients. In comparison to prior analyses, this meta-analysis added new data from FAIR-HF2, used a harmonized and robust Bayesian approach and included individual participant data from five trials. Patients assigned to i.v. iron, compared with those assigned to placebo, had lower rates for the composite endpoint of recurrent HF hospitalizations and cardiovascular mortality at 12 months (risk ratio (RR) = 0.72 (95% confidence interval (CI) = 0.55-0.89)) and for the complete length of follow-up (RR = 0.81 (95% CI = 0.63-0.97)). Each component of the primary endpoint contributed to the beneficial effect of i.v. iron at both 12 months and the complete length of follow-up: recurrent HF hospitalizations (RR = 0.69 (95% CI = 0.48-0.88) and RR = 0.78 (95% CI = 0.55-0.98), respectively) and cardiovascular mortality (hazard ratio (HR) = 0.80 (95% CI = 0.61-1.03) and HR = 0.87 (95% CI = 0.73-1.04), respectively). All-cause mortality at 12 months and for the complete length of follow-up (HR = 0.82 (95% CI = 0.65-1.03)) and HR = 0.92 (95% CI = 0.80-1.07), respectively, indicated the overall safety of i.v. iron treatment. Treatment effects were greatest in the first year after randomization when the doses of i.v. iron provided are highest. These findings suggest that treating iron deficiency in patients with HF significantly reduces cardiovascular events and also suggests further investigation of optimal dosing of i.v. iron.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: S.D.A. reports grants and personal fees from CSL Vifor and Abbott Vascular, and personal fees for consultancies, trial committee work and/or lectures from Actimed, AstraZeneca, Bayer, Bioventrix, Boehringer Ingelheim, Brahms, Cardiac Dimensions, Cardior, Cordio, CVRx, Cytokinetics, Edwards, Farraday Pharmaceuticals, GSK, HeartKinetics, Impulse Dynamics, Medtronic, Novartis, Novo Nordisk, Occlutech, Pfizer, Regeneron, Relaxera, Repairon, Scirent, Sensible Medical, Servier, Vectorious and V-Wave. He is the named co-inventor of two patent applications regarding MR-proANP (nos. DE 102007010834 and DE 102007022367), but he does not benefit personally from the related issued patents. M.K. is supported by a clinician scientist professorship grant from the Else Kroener-Fresenius-Foundation. He reports grant and nonfinancial support from Adrenomed AG and CSL Vifor, as well as personal fees from Adrenomed AG, Sphingotec, CSL Vifor, Daiichi Sankyo, Pharmacosmos and 4TEEN4, and is a part-time employee of 4TEEN4 Pharmaceuticals GmbH. R.J.M. received research support and honoraria from Abbott, Alleviant Medical, American Regent, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Cytokinetics, Fast BioMedical, Gilead, Innolife, Eli Lilly, Lexicon, Medtronic, Medable, Merck, Novartis, Novo Nordisk, Pfizer, Pharmacosmos, Relypsa, Reprieve Cardiovascular, Respicardia, Roche, Rocket Pharmaceuticals, Sanofi, Verily, CSL Vifor, Windtree Therapeutics and Zoll. P.P. received consulting fees from Boehringer Ingelheim, AstraZeneca, CSL Vifor Pharma, Servier, Novartis, Bayer, MSD, Novo Nordisk, Pharmacosmos, Moderna and WhiteSwell. He also received honoraria from Boehringer Ingelheim, AstraZeneca, CSL Vifor Pharma, Amgen, Servier, Novartis, Bayer, Pfizer and Abbott Vascular for lectures, presentations, speakers’ bureaus, manuscript writing or educational events. J.B. reports consulting fees from Abbott, American Regent, Amgen, Applied Therapeutic, AskBio, Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardiac Dimension, Cardiocell, Cardior, Cardiorem, CSL Bearing, CVRx, Cytokinetics, Daxor, Edwards, Element Science, Faraday, Foundry, G3P, Innolife, Impulse Dynamics, Imbria, Inventiva, Ionis, Lexicon, Lilly, LivaNova, Janssen, Medtronics, Merck, Occlutech, Owkin, Novartis, Novo Nordisk, Pfizer, Pharmacosmos, Pharmain, Pfize, Prolaio, Regeneron, Renibus, Roche, Salamandra, Sanofi, SC Pharma, Secretome, Sequana, SQ Innovation, Tenex, Tricog, Ultromics, CSL Vifor and Zoll, and honoraria from Novartis, Boehringer Ingelheim-Lilly, AstraZeneca, Impulse Dynamics and CSL Vifor. M.S.K. received fees from Bayer and Novartis. K.M.T. reported no competing interests. P.R.K. reports grant or research support from Pharmacosmos and consulting fees or honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, CSL Vifor, Novartis and Pharmacosmos. A.F.H. reported receiving grants from Boehringer Ingleheim, Cytokinetics, Novartis, Novo Nordisk, Verily, Bayer, Amgen and AstraZeneca and receiving personal fees from Boston Scientific, Bristol Myers Squibb, Eidos Therapeutics, GlaxoSmithKline, Intellia, Intercept, MyoKardia, Prolaio and TikkunLev Therapeutics. H.M. reported no competing interests. F.W.R. received grants from the National Institutes of Health, PCORI, BMS, AstraZeneca, American Regent, the Gates Foundation and Eidos and consulting fees from Janssen, Clover, Doctor Evidence and Intercept. He also participated on Data Safety Monitoring Boards for Lilly, AstraZeneca, Merck, Gilead, Novartis, Icosavax, Sanofi, UCB, Amgen, Biogen, BMS, Pulmocide, Alkermes and Diurnal. He had an unpaid leadership role for the Frontier Science Foundation. He has stock or stock options for GSK, Clover, Athira, Doctor Evidence, DataVant, Spencer Health Solutions and Adaptic Health. M.P. and C.R. reported no competing interests. J.G.F.C. received research funding from Bristol Myers Squibb, CSL Vifor, British Heart Foundation and Pharmacosmos, consulting fees from Pharmacosmos, CSL Vifor and Biopeutics, a personal honorarium from Pharmacosmos and ABBOTT, travel support from Pharmacosmos, participated on advisory boards of Medtronic, ADAPT-CRT, CMR-Guide and PROTECT-HF, and has stocks or stock options in HeartFelt (noninvasive monitoring) and Viscardia (synchronous diaphragmatic pacing). T.F. reports payments to institution from Abbott, grants from Deutsche Forschungsgemeinschaft, Federal Joint Committee (G-BA) and the European Commission, consulting fees from Actimed, Bayer, BMS, CSLBehring, Daiichi Sankyo, Galapagos, Immunic, KyowaKirin, LivaNova, Minoryx, Novartis, RECARDIO, Relaxera, Roche, Servier, Viatris and CSL Vifor, payments from Fresenius Kabi and PINK gegen Brustkrebs, and is a trial data monitoring committee member of Aslan, Bayer, BiosenseWebster, Enanta, Galapagos, IQVIA, Novartis, PPD, Recordati, Roche and VICO Therapeutics and a trial steering committee member of CSLBehring.
Figures








References
-
- Wahid, M. et al. Iron deficiency, anemia, and iron supplementation in patients with heart failure: a population-level study. Circ. Heart Fail.17, e011351 (2024). - PubMed
-
- Masini, G. et al. Criteria for iron deficiency in patients with heart failure. J. Am. Coll. Cardiol.79, 341–351 (2022). - PubMed
-
- Aland, S. C. et al. Exercise capacity, iron deficiency and depressive symptoms in patients with asymptomatic chronic systolic heart failure. Glob. Cardiol.10.4081/cardio.2024.39 (2024).
-
- McDonagh, T. A., ESC Scientific Document Group et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail.24, 4–131 (2022). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
