

Adoptive Transfer of T Cells as a Potential Therapeutic Approach in the Bleomycin-Injured Mouse Lung
- PMID: 40159455
- PMCID: PMC11955259
- DOI: 10.1002/jgm.70018
Adoptive Transfer of T Cells as a Potential Therapeutic Approach in the Bleomycin-Injured Mouse Lung
Abstract
Background: Idiopathic pulmonary fibrosis (IPF) is a lethal disease with an unknown etiology and complex pathophysiology that are not fully understood. The disease involves intricate cellular interplay, particularly among various immune cells. Currently, there is no treatment capable of reversing the fibrotic process or aiding lung regeneration. Hepatocyte growth factor (HGF) has demonstrated antifibrotic properties, whereas the adoptive transfer of modified T cells is a well-established treatment for various malignancies. We aimed to understand the dynamics of T cells in the progression of lung fibrosis and to study the therapeutic benefit of adoptive T cell transfer in a bleomycin-injured mouse lung (BLM) model.
Methods: T cells were isolated from the spleen of naïve mice and transfected in vitro with mouse HGF plasmid and were administered intratracheally to the mice lungs 7 days post-bleomycin injury to the lung. Lung tissue and bronchoalveolar lavage were collected and analyzed using flow cytometry, histology, qRT-PCR, ELISA, and hydroxyproline assay.
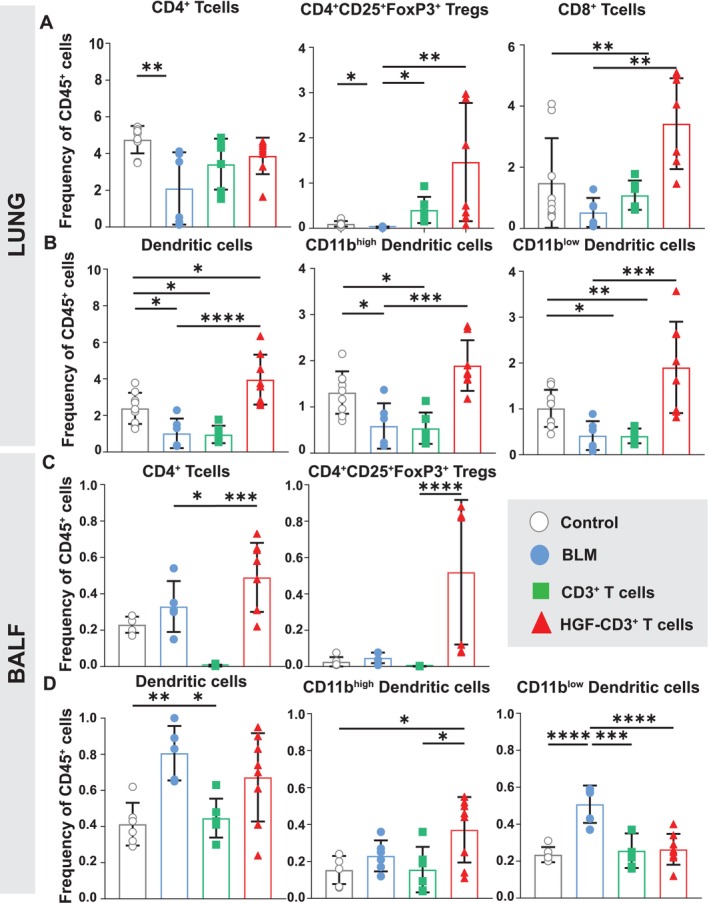
Results: Our findings demonstrate the successful T cell therapy of bleomycin-induced lung injury through the adoptive transfer of HGF-transfected T cells in mice. This treatment resulted in decreased collagen deposition and a balancing of immune cell exhaustion and cytokine homeostasis compared with untreated controls. In vitro testing showed enhanced apoptosis in myofibroblasts induced by HGF-overexpressing T cells.
Conclusions: Taken together, our data highlight the great potential of adoptive T cell transfer as an emerging therapy to counteract lung fibrosis.
Keywords: T cells homeostasis; adoptive transfer; bleomycin lung injury and fibrosis; immune exhaustion.
© 2025 The Author(s). The Journal of Gene Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Finnerty J. P., Ponnuswamy A., Dutta P., Abdelaziz A., and Kamil H., “Efficacy of Antifibrotic Drugs, Nintedanib and Pirfenidone, in Treatment of Progressive Pulmonary Fibrosis in Both Idiopathic Pulmonary Fibrosis (IPF) and Non‐IPF: A Systematic Review and Meta‐Analysis,” BMC Pulmonary Medicine 21 (2021): 411, 10.1186/S12890-021-01783-1. - DOI - PMC - PubMed
