

Preclinical extracellular matrix-based treatment strategies for myocardial infarction: a systematic review and meta-analysis
- PMID: 40159511
- PMCID: PMC11955565
- DOI: 10.1038/s43856-025-00812-y
Preclinical extracellular matrix-based treatment strategies for myocardial infarction: a systematic review and meta-analysis
Abstract
Background: Administrating extracellular matrix (ECM) to restore cardiac function post-myocardial infarction (MI) shows promise, however study variability obscures its true impact. We therefore conducted a systematic review and meta-analysis of preclinical studies to assess the effects of ECM treatments on cardiac function and tissue homeostasis post-MI.
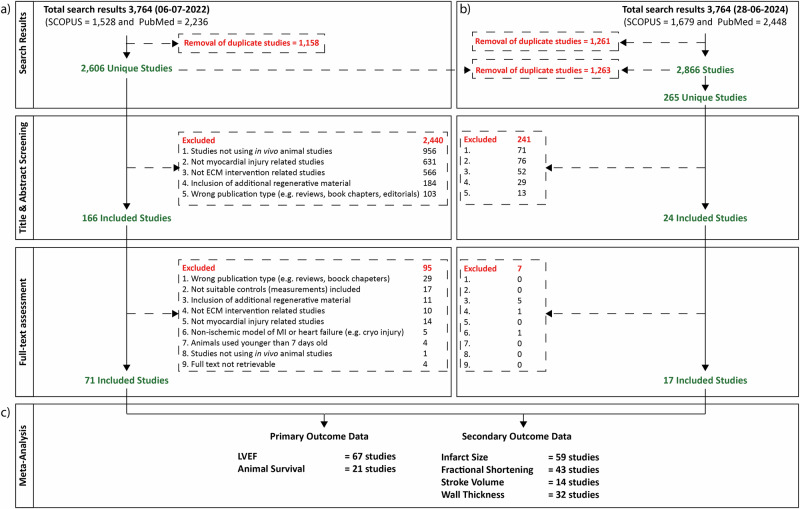
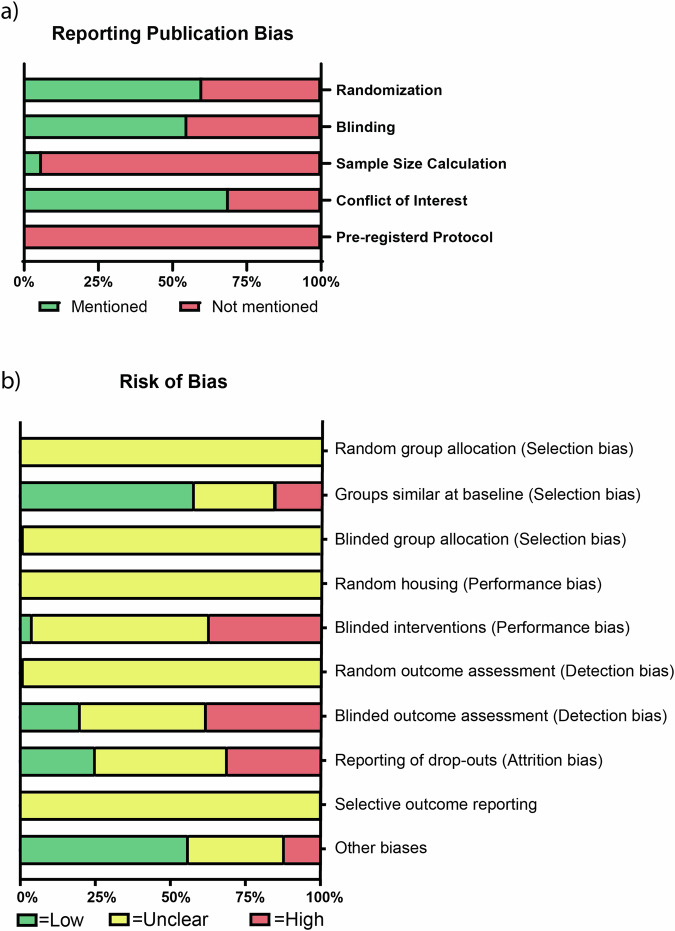
Methods: We searched PubMed and SCOPUS from inception to June 28, 2024, for animal studies describing ECM treatment post-MI (pre-registered on PROSPERO, CRD42022368400). Random effects meta-analyses compared ECM treatment to controls regarding left ventricular ejection fraction (LVEF), fractional shortening, infarct size, stroke volume, and left ventricular wall thickness. Subgroup analyses examined the influence of sex, species, ECM source, and administration method. Funnel plots and Egger's regression assessed publication bias.
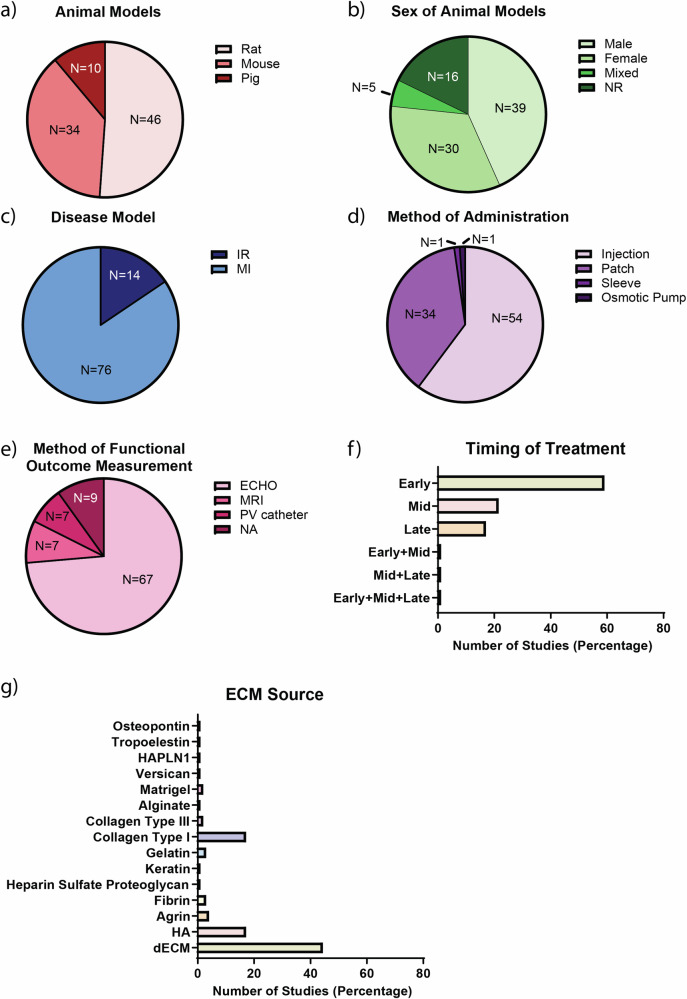
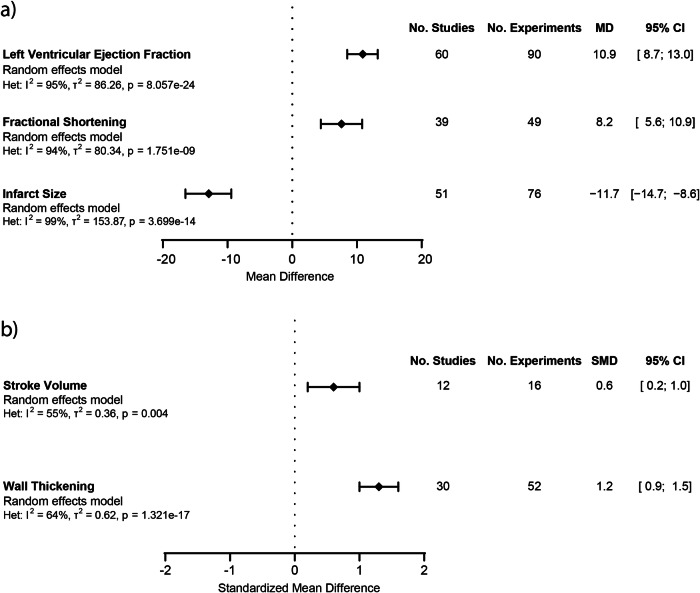
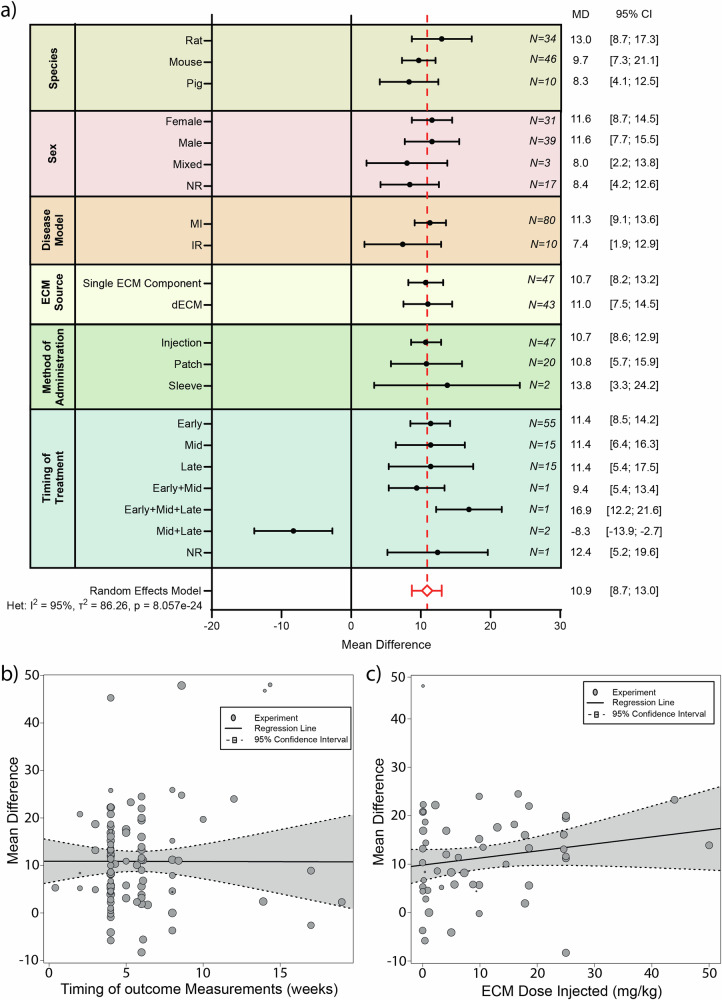
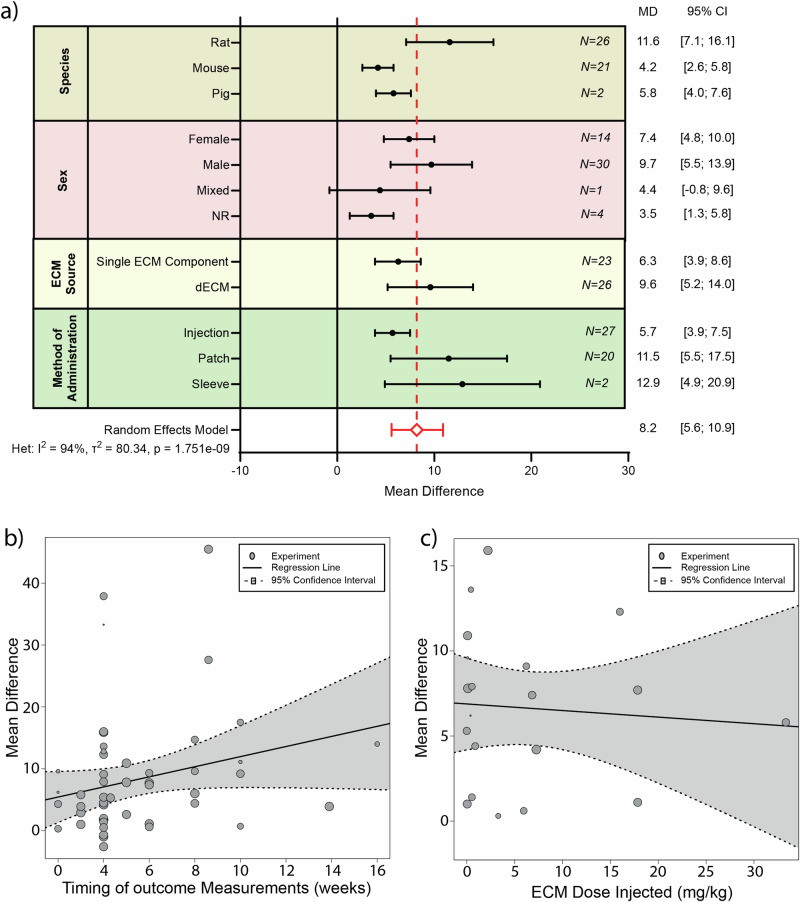
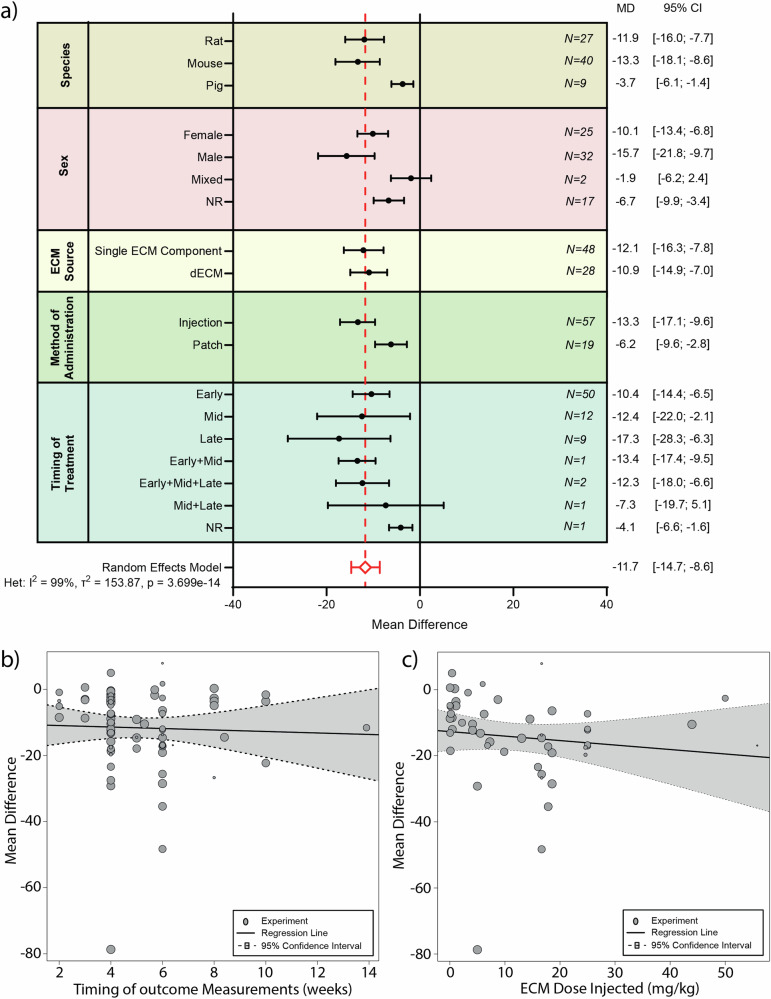
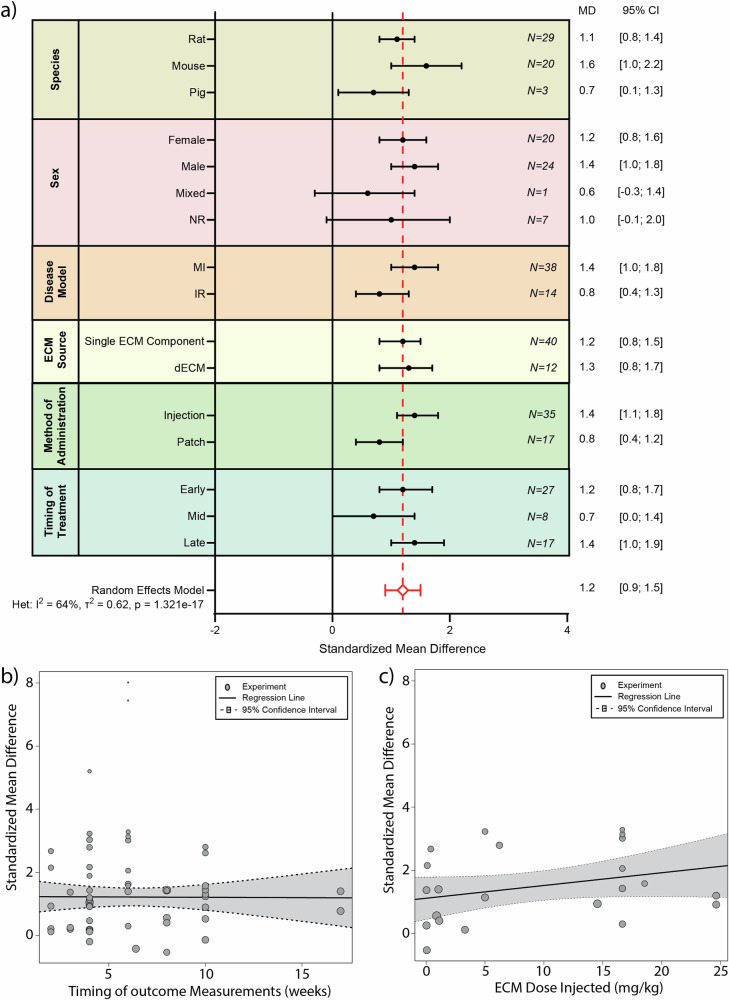
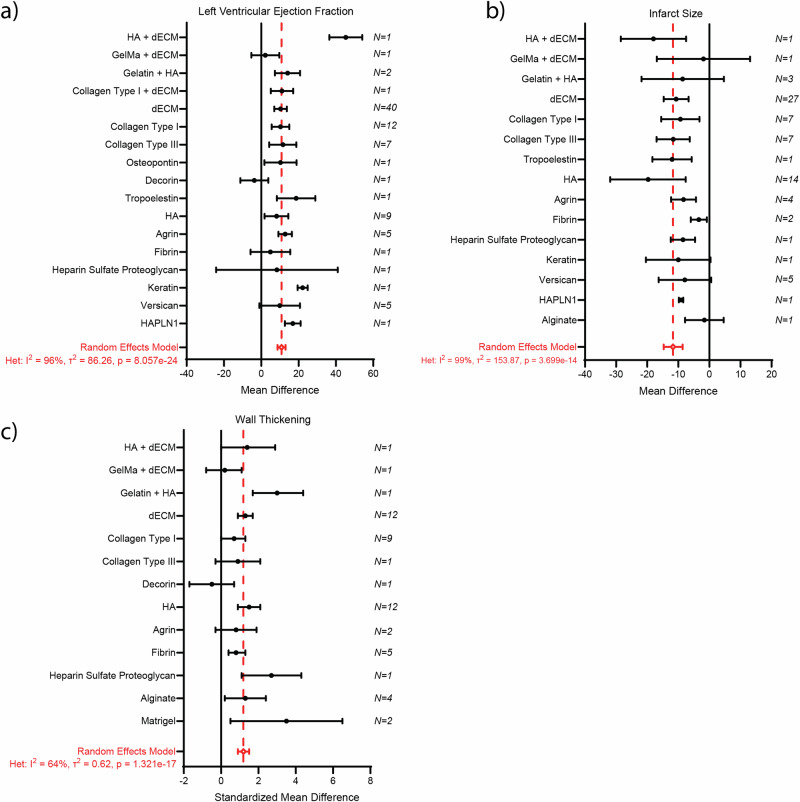
Results: We identify 88 articles which meet our inclusion criteria. These studies describe the use of rats (51%), mice (38%), and pigs (11%). 44% of studies use males, 34% females, 5% both sexes, and 17% did not report sex. Most studies employ permanent MI models (85%) over ischemia reperfusion models (15%), and deliver ECM via intramyocardial injection (59%), cardiac patch (39%), cardiac sleeve (1%), or osmotic pump (1%). Our meta-analysis demonstrates that ECM treatment significantly improves LVEF (MD: 10.9%, 95% CI: [8.7%;13.0%]; p = 8.057e-24), fractional shortening (MD: 8.2%, 95% CI: [5.6%; 10.9%]; p = 1.751e-09), stroke volume (SMD 0.6, 95% CI: [0.2;1.0], p = 0.004), left ventricular wall thickening (SMD 1.2, 95% CI: [0.9; 1.5], p = 1.321e-17), while reducing infarct size (-11.7%, 95% CI: [-14.7%;-8.6%], p = 3.699e-14). We find no significant differences between the various subgroups and no indication of publication bias.
Conclusions: ECM-based treatments significantly enhance cardiac function and tissue homeostasis in preclinical post-MI models, supporting further research toward clinical translation.
Plain language summary
A heart attack leads to loss of cells that control heartbeat and the formation of unhealthy scar tissue that can cause heart failure. Traditional treatment strategies focusing on replacing cell loss show limited improvement in heart function. Recent approaches to restore the balance in heart tissue by supplying a healthy support structure, known as the extracellular matrix, show promising results. However, differences in study design make it hard to determine effectiveness across groups. By analysing studies in animal models thoroughly, we find that treatments involved in supplying healthy support structure significantly improve heart function in preclinical models by improving the heart’s ability to pump blood and reduce scar tissue formation, regardless of species, sex, or the source of the extracellular matrix. These findings provide a strong foundation for future research focused on improving the support matrix of the heart to restore heart function.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Bioactive scaffolds in stem-cell-based therapies for cardiac repair: protocol for a meta-analysis of randomized controlled preclinical trials in animal myocardial infarction models.Syst Rev. 2018 Dec 5;7(1):225. doi: 10.1186/s13643-018-0845-z. Syst Rev. 2018. PMID: 30518435 Free PMC article.
-
Possible mechanism by which renal sympathetic denervation improves left ventricular remodelling after myocardial infarction.Exp Physiol. 2016 Feb;101(2):260-71. doi: 10.1113/EP085302. Epub 2015 Dec 16. Exp Physiol. 2016. PMID: 26556551
-
Hypoxic Stem Cell-Derived Extracellular Vesicles for Cardiac Repair in Preclinical Animal Models of Myocardial Infarction: A Meta-Analysis.Stem Cells Dev. 2021 Sep 15;30(18):891-907. doi: 10.1089/scd.2021.0084. Epub 2021 Aug 13. Stem Cells Dev. 2021. PMID: 34271845
-
Injectable hydrogel-based combination therapy for myocardial infarction: a systematic review and Meta-analysis of preclinical trials.BMC Cardiovasc Disord. 2024 Feb 21;24(1):119. doi: 10.1186/s12872-024-03742-0. BMC Cardiovasc Disord. 2024. PMID: 38383333 Free PMC article.
-
Extracellular Vesicles as a Cell-free Therapy for Cardiac Repair: a Systematic Review and Meta-analysis of Randomized Controlled Preclinical Trials in Animal Myocardial Infarction Models.Stem Cell Rev Rep. 2022 Mar;18(3):1143-1167. doi: 10.1007/s12015-021-10289-6. Epub 2022 Feb 2. Stem Cell Rev Rep. 2022. PMID: 35107768
References
-
- Tsao, C. W. et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation145, e153–e639 (2022). - PubMed
-
- McDonagh, T. A. et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J.42, 3599–3726 (2021). - PubMed
-
- Ye, L. et al. Early Regenerative Capacity in the Porcine Heart. Circulation138, 2798–2808 (2018). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
