

Spetzler-martin grade IV cerebral arteriovenous malformations in adult patients: a propensity-score matched analysis of resection and stereotactic radiosurgery
- PMID: 40159532
- PMCID: PMC11955433
- DOI: 10.1007/s10143-025-03465-6
Spetzler-martin grade IV cerebral arteriovenous malformations in adult patients: a propensity-score matched analysis of resection and stereotactic radiosurgery
Abstract
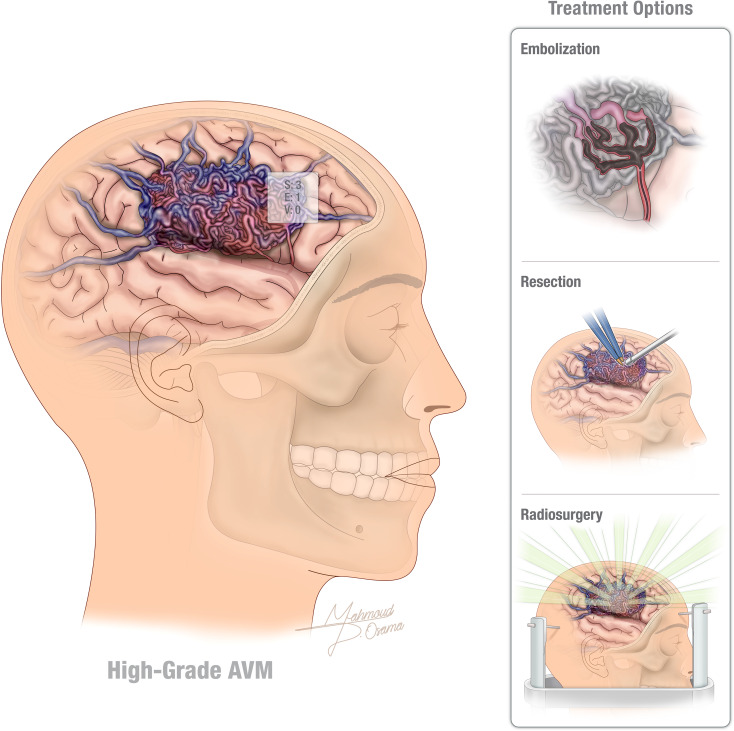
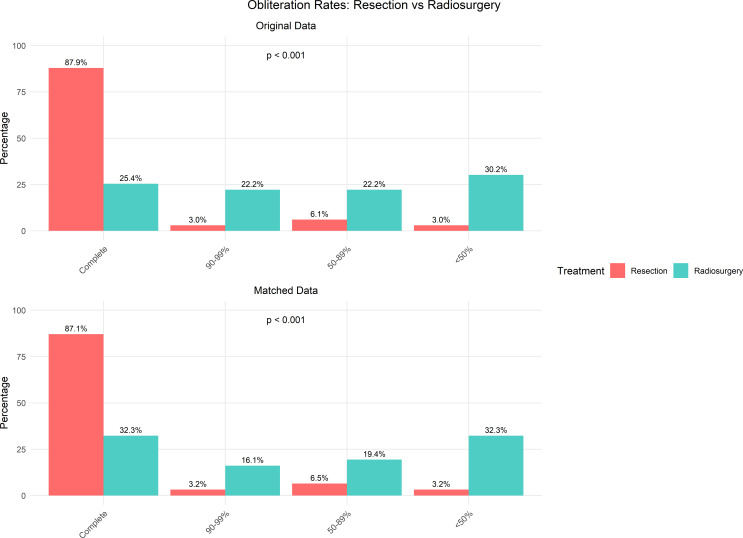
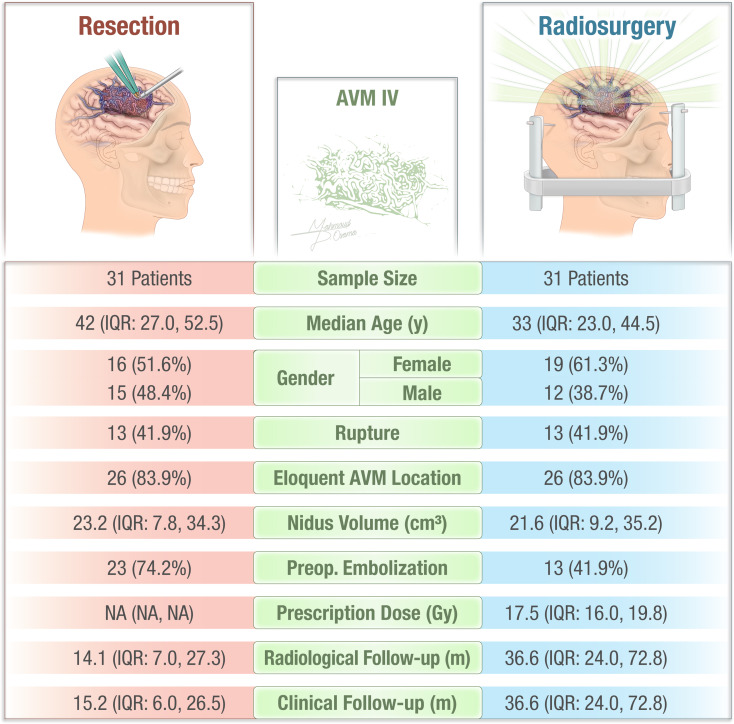
Spetzler-Martin Grade IV arteriovenous malformations (AVMs) are challenging due to high risks associated with both treatment and natural progression. This study compares the outcomes of microsurgical resection and stereotactic radiosurgery (SRS) in high-grade AVMs, analyzing obliteration rates, complications, and functional outcomes. A retrospective cohort of 96 patients treated with either microsurgical resection (33 patients) or SRS (63 patients) was analyzed. Propensity-score matching was employed to account for baseline variables such as AVM size (cm), preoperative embolization and rupture status. Primary endpoints included AVM obliteration, complication rates, and modified Rankin Scale (mRS) scores. After matching, 31 patients per group were analyzed. Microsurgical resection achieved significantly higher obliteration rates (87.1%) compared to SRS (32.3%, p < 0.001). In the matched SRS cohort (n = 31), the actuarial obliteration rates were 11% (95% CI: 0-22%) at 1 year, 17% (95% CI: 0-31%) at 3 years, and 43% (95% CI: 13-63%) at 5 years post-treatment. Complication rates were similar (32.3% resection, 38.7% SRS, p = 0.6). Functional outcomes in terms of improvement in modified Rankin Scale (mRS) scores were observed in 50.0% of microsurgery patients and 41.4% of SRS patients. However, the absolute number of patients improving was similar (13 vs. 12), and the microsurgery group had more cases of worsening mRS scores compared to the SRS group (4 vs. 2). The difference was not statistically significant (p = 0.4). Microsurgical resection offers superior obliteration rates for high-grade AVMs with comparable complication risks to SRS. SRS remains a valuable alternative for select patients, particularly those ineligible for resection. Future research should focus on optimizing multimodal treatment approaches. Clinical trial number Not applicable.
Keywords: AVM obliteration; Cerebral arteriovenous malformations; Complication rates and functional outcomes; Resection; Spetzler-martin grade IV; Stereotactic radiosurgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This retrospective multicenter clinical cohort study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of University of Virginia Hospital. Due to the retrospective nature of the study, the requirement for informed consent was waived by the IRB. All patient data were anonymized and de-identified prior to analysis to ensure patient confidentiality. Human ethics and consent to participate: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Jayaraman MV, Marcellus ML, Do HM et al (Feb 2007) Hemorrhage rate in patients with Spetzler-Martin grades IV and V arteriovenous malformations: is treatment justified? Stroke. 38(2):325–329. 10.1161/01.STR.0000254497.24545.de - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
