

Systematic review and meta-analysis comparing extraperitoneal and transperitoneal routes of colostomy-related complications
- PMID: 40162385
- PMCID: PMC11948114
- DOI: 10.4240/wjgs.v17.i3.98947
Systematic review and meta-analysis comparing extraperitoneal and transperitoneal routes of colostomy-related complications
Abstract
Background: Complications associated with stomas-including parastomal hernia (PSH), prolapse, mucocutaneous separation, and stoma retraction-provide considerable postoperative challenges for colostomy patients. Selecting between extraperitoneal colostomy (EPC) and transperitoneal colostomy (TPC) pathways is therefore essential for mitigating these complications.
Aim: To analyze the existing data regarding the efficacy of EPC compared to TPC in reducing stoma-related complications post-colostomy.
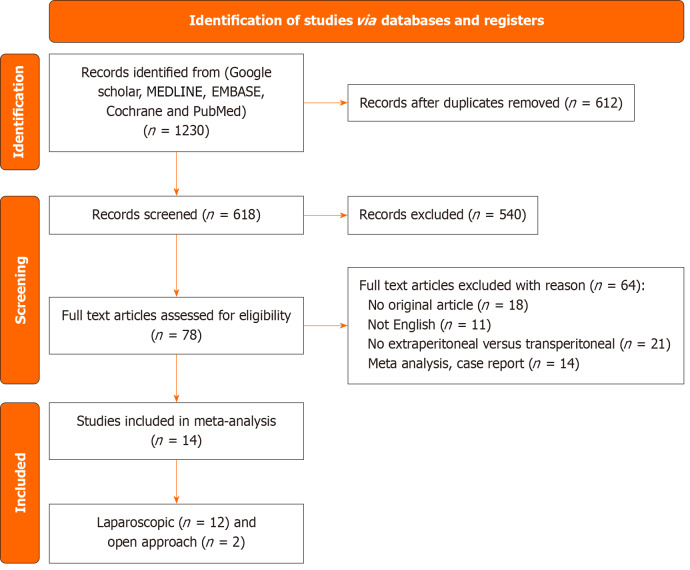
Methods: PubMed, Google Scholar, EMBASE, MEDLINE, and the Cochrane Library were adopted to uncover pertinent papers in which EPC and TPC approaches were compared. We then conducted a meta-analysis using RevMan 5.4.1.
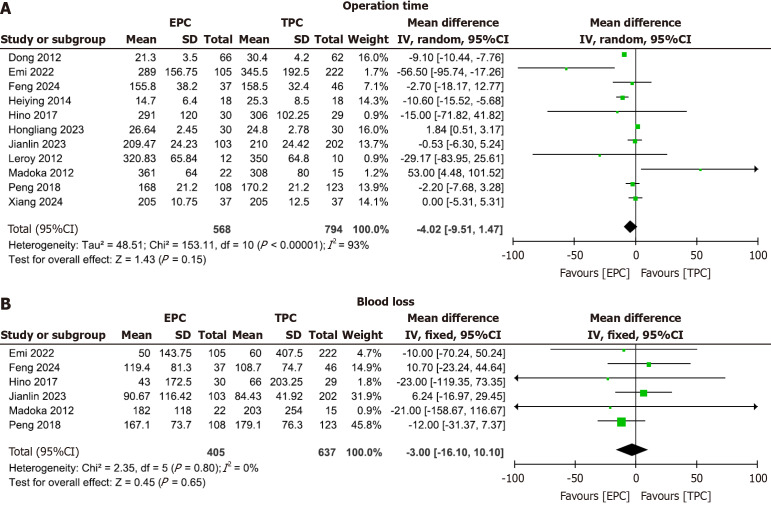
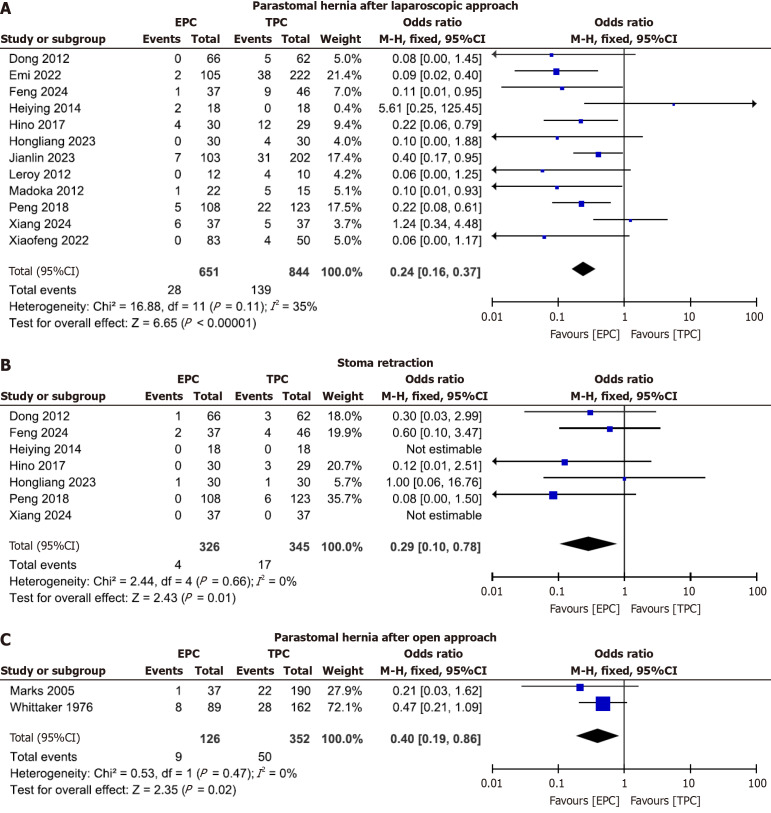
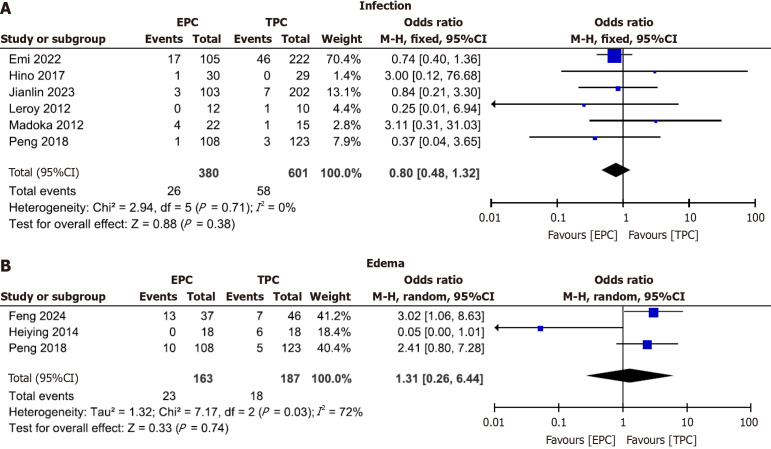
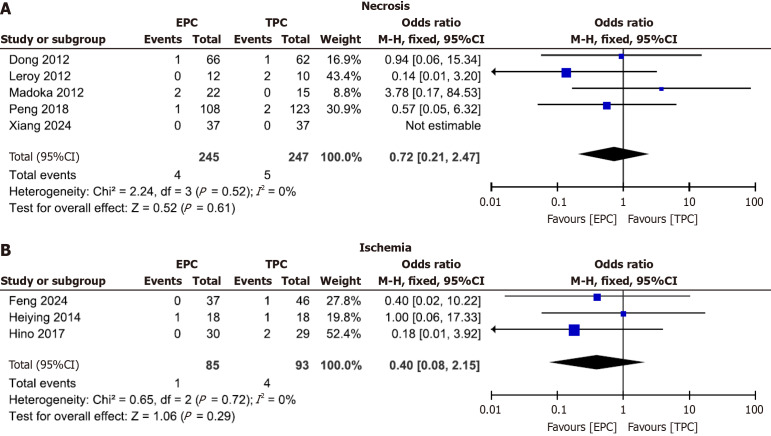
Results: Both laparoscopic (Lap) and open approaches showed a reduced incidence of PSH in EPC relative to TPC (P < 0.00001 and P = 0.02 respectively). In addition, Lap EPC depicted a lesser incidence of prolapse, mucocutaneous separation, and stoma retraction (P = 0.007, P = 0.03, and P = 0.01, respectively) compared to Lap TPC. However, EPC and TPC did not differ with respect to operation time, blood loss, edema, ischemia, necrosis, or infection after the LAP approach.
Conclusion: The extraperitoneal approach may provide benefits in minimizing some stoma-related problems such as PSH, prolapse, mucocutaneous separation, and stoma retraction after colostomy surgery.
Keywords: Abdominoperineal resection; Colostomy; Extraperitoneal; Parastomal hernia; Transperitoneal.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394:1467–1480. - PubMed
-
- Simillis C, Baird DL, Kontovounisios C, Pawa N, Brown G, Rasheed S, Tekkis PP. A Systematic Review to Assess Resection Margin Status After Abdominoperineal Excision and Pelvic Exenteration for Rectal Cancer. Ann Surg. 2017;265:291–299. - PubMed
-
- Gopall J, Shen XF, Cheng Y. Current status of laparoscopic total mesorectal excision. Am J Surg. 2012;203:230–241. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
