

AI-Quantitative CT Coronary Plaque Features Associate With a Higher Relative Risk in Women: CONFIRM2 Registry
- PMID: 40162910
- PMCID: PMC12173162
- DOI: 10.1161/CIRCIMAGING.125.018235
AI-Quantitative CT Coronary Plaque Features Associate With a Higher Relative Risk in Women: CONFIRM2 Registry
Abstract
Background: Coronary plaque features are imaging biomarkers of cardiovascular risk, but less is known about sex-specific patterns in their prognostic value. This study aimed to define sex differences in the coronary atherosclerotic phenotypes assessed by artificial intelligence-based quantitative computed tomography (AI-QCT) and the associated risk of major adverse cardiovascular events (MACEs).
Methods: Global multicenter registry including symptomatic patients with suspicion of coronary artery disease referred for coronary computed tomography angiography. AI-QCT analyzed 16 coronary artery disease features. The primary end point was MACE defined as death, myocardial infarction, late revascularization, cerebrovascular events, unstable angina, and congestive heart failure.
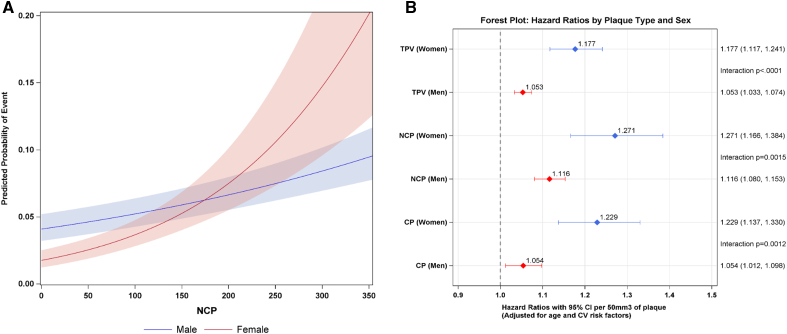
Results: Among 3551 patients (mean age, 59±12 years; 49.5% women), MACE occurred in 3.2% of women and 6.1% of men during an average follow-up of 4.8±2.2 years. The AI-QCT features total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume were significantly higher in men (P<0.001), and high-risk plaques were more prevalent (9.2% versus 2.5%; P<0.0001). Independent of age and cardiovascular risk factors, the AI-QCT-derived features of total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume conferred a higher relative risk of MACE in women than men. For every 50-mm3 increase in total plaque volume, relative risk increased by 17.7% (95% CI, 1.12-1.24) in women versus 5.3% (95% CI, 1.03-1.07) in men (Pinteraction<0.001); for noncalcified plaque, relative risk increased by 27.1% (95% CI, 1.17-1.38) versus 11.6% (95% CI, 1.08-1.15; Pinteraction=0.0015); and for calcified plaque, relative risk increased by 22.9% (95% CI, 1.14-1.33) versus 5.4% (95% CI, 1.01-1.10; Pinteraction=0.0012), respectively. Similarly, for percentage atheroma volume, the risk was higher in women. The findings remained unchanged when restricted to a secondary composite end point (death and myocardial infarction).
Conclusions: The AI-QCT plaque features, total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume, conferred a higher relative MACE risk in women and may prompt more aggressive antiatherosclerotic therapy and reinforced preventive interventions.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT04279496.
Keywords: artificial intelligence; atherosclerosis; computed tomography; computed tomography angiography; coronary artery disease; women’s health.
Conflict of interest statement
The authors declare the following financial interests/personal relationships that may be considered potential competing interests. Dr van Rosendael is a member of the Cleerly Scientific Advisory Board. Dr Pontone received an honorarium as a speaker/consultant and an institutional research grant from GE Healthcare, Bracco, Medtronic, and Novartis. Dr Buechel reports receiving speaking honoraria from GE Healthcare, Pfizer, Gilead, and IBA. Dr Gräni received funding from the Swiss National Science Foundation, InnoSuisse, the CAIM Foundation, the GAMBIT Foundation, and the Novartis Foundation for biomedical research, outside of the submitted work. Dr Choi is a consultant for Siemens, holds equity in Cleerly, and receives grant support from the George Washington Heart and Vascular Institute. Dr Rochitte reports receiving speaking honoraria for Pfizer, Edwards, GE, and Manole. Dr Khalique is a consultant for Edwards, Croivalve, and Restore Medical, holds equity in Triflo, and received honoraria for educational programs from Heartflow. Udo Hoffmann is an employee and equity holder in Cleerly, Inc, and received honoraria from Stanford University, Clinical Cardiovascular Sciences, Rapid AI, and MedTrace. Dr Danad is a member of the Cleerly Scientific Advisory Board. Dr Marques is a consultant for Cleerly, Inc. The other authors report no conflicts.
Figures

Comment in
-
Unfolding Evidence on Risk Stratification in Women Using Quantitative Atherosclerotic Plaque Measurements.Circ Cardiovasc Imaging. 2025 Jun;18(6):e018438. doi: 10.1161/CIRCIMAGING.125.018438. Epub 2025 May 30. Circ Cardiovasc Imaging. 2025. PMID: 40444358 No abstract available.
References
-
- Martin SS, Aday AW, Allen NB, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Bansal N, Beaton AZ, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Committee. 2025 Heart Disease and Stroke Statistics: a report of US and global data from the American Heart Association. Circulation. 2025;151:e41–e660. doi: 10.1161/CIR.0000000000001303 - PubMed
-
- Pagidipati NJ, Coles A, Hemal K, Lee KL, Dolor RJ, Pellikka PA, Mark DB, Patel MR, Litwin SE, Daubert MA, et al. ; PROMISE Investigators. Sex differences in management and outcomes of patients with stable symptoms suggestive of coronary artery disease: insights from the PROMISE trial. Am Heart J. 2019;208:28–36. doi: 10.1016/j.ahj.2018.11.002 - PMC - PubMed
-
- Reynolds HR, Shaw LJ, Min JK, Spertus JA, Chaitman BR, Berman DS, Picard MH, Kwong RY, Bairey-Merz CN, Cyr DD, et al. ; ISCHEMIA Research Group. Association of sex with severity of coronary artery disease, ischemia, and symptom burden in patients with moderate or severe ischemia: secondary analysis of the ISCHEMIA randomized clinical trial. JAMA Cardiol. 2020;5:773–786. doi: 10.1001/jamacardio.2020.0822 - PMC - PubMed
-
- van Rosendael SE, Bax AM, Lin FY, Achenbach S, Andreini D, Budoff MJ, Cademartiri F, Callister TQ, Chinnaiyan K, Chow BJW, et al. Sex and age-specific interactions of coronary atherosclerotic plaque onset and prognosis from coronary computed tomography. Eur Heart J Cardiovasc Imaging. 2023;24:1180–1189. doi: 10.1093/ehjci/jead094 - PMC - PubMed
