

Can posterior fossa decompression alone effectively treat Chiari malformation type I patients with even severe syringes? Illustrative cases
- PMID: 40163896
- PMCID: PMC11959644
- DOI: 10.3171/CASE24777
Can posterior fossa decompression alone effectively treat Chiari malformation type I patients with even severe syringes? Illustrative cases
Abstract
Background: The benefit of posterior fossa decompression (PFD) alone (without duraplasty) for Chiari malformation type I (CM-I) remains controversial. Many neurosurgeons still open the dura when a syrinx is present, particularly for what appears to be a severe syrinx. Based on the existing literature, the authors hypothesized that even a severe syrinx would respond well to a PFD alone.
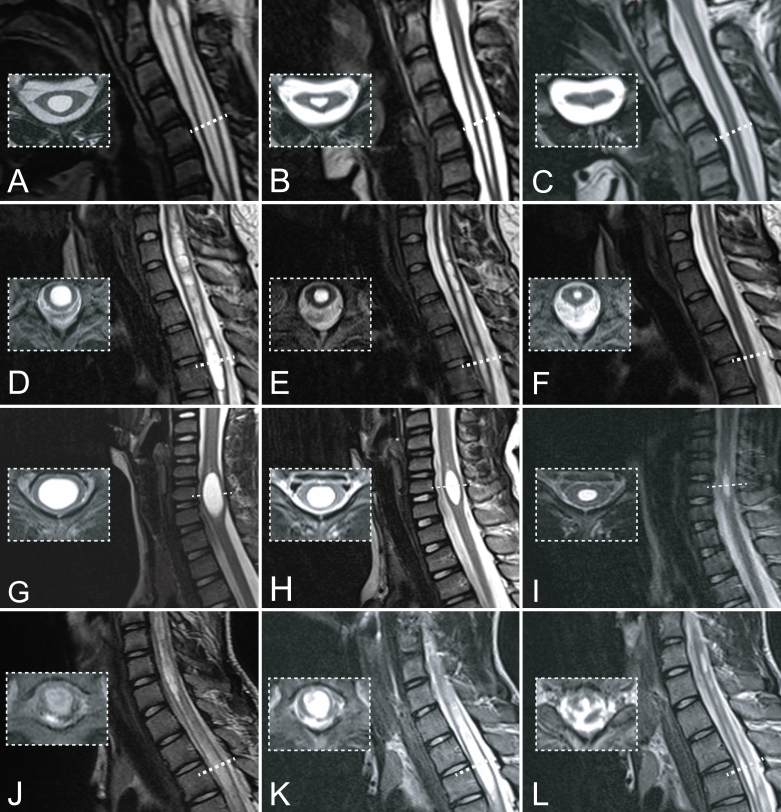
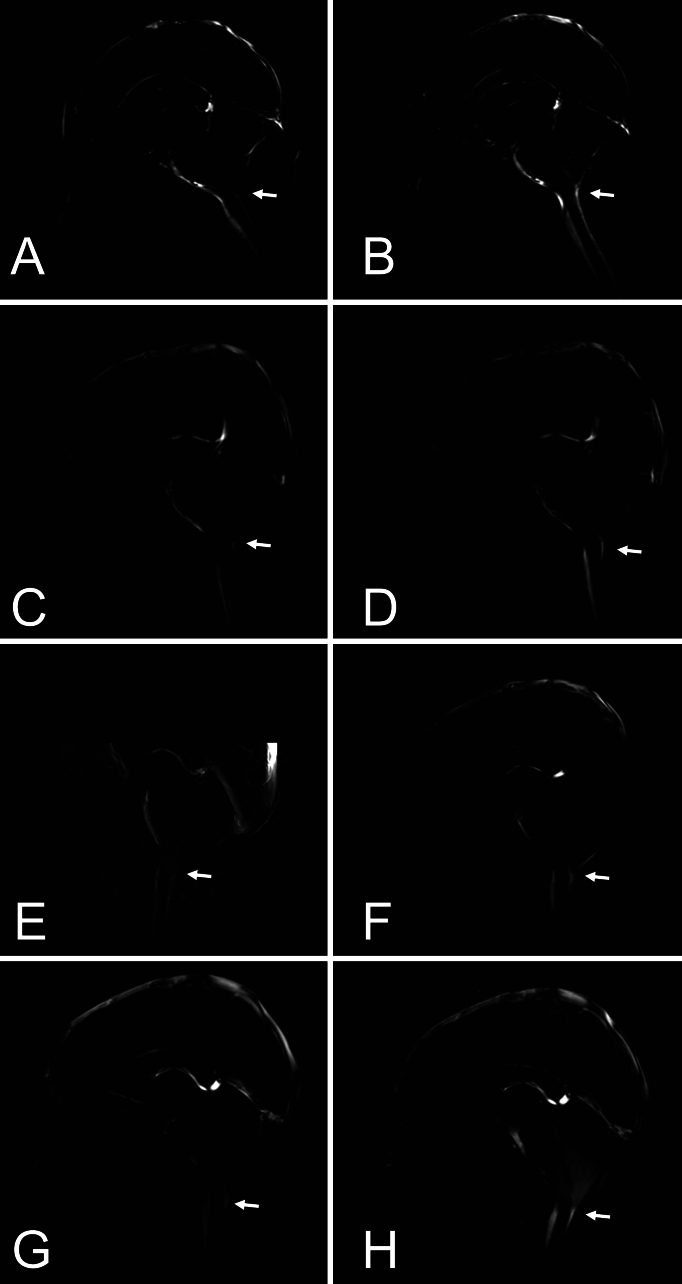
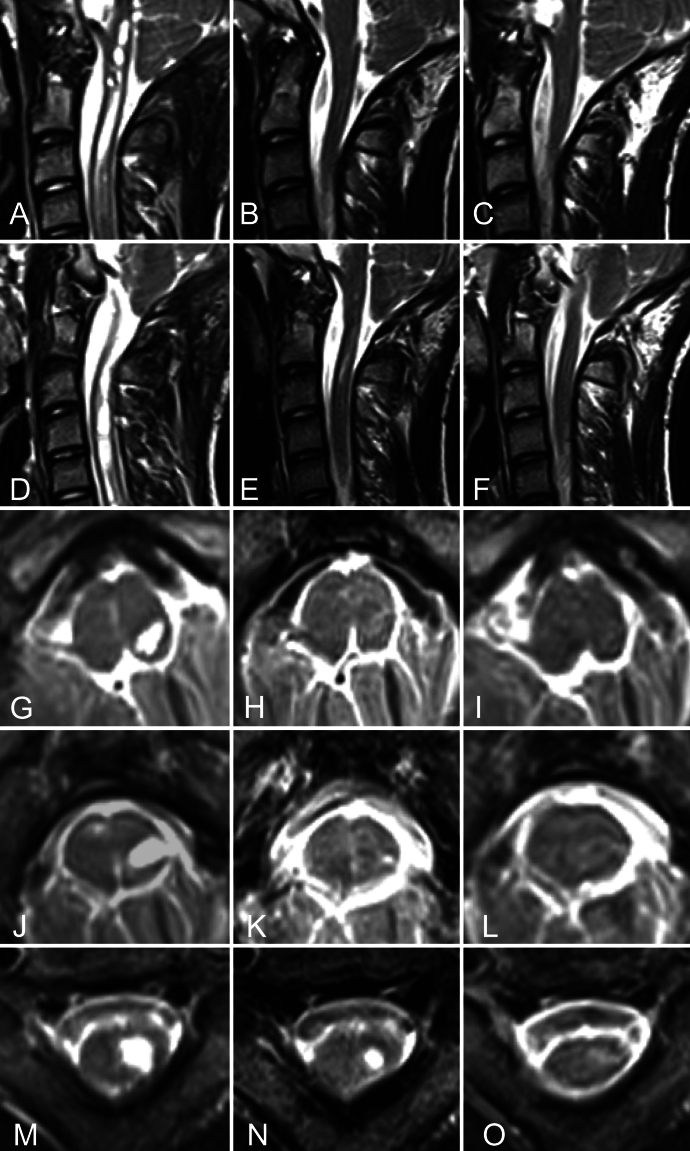
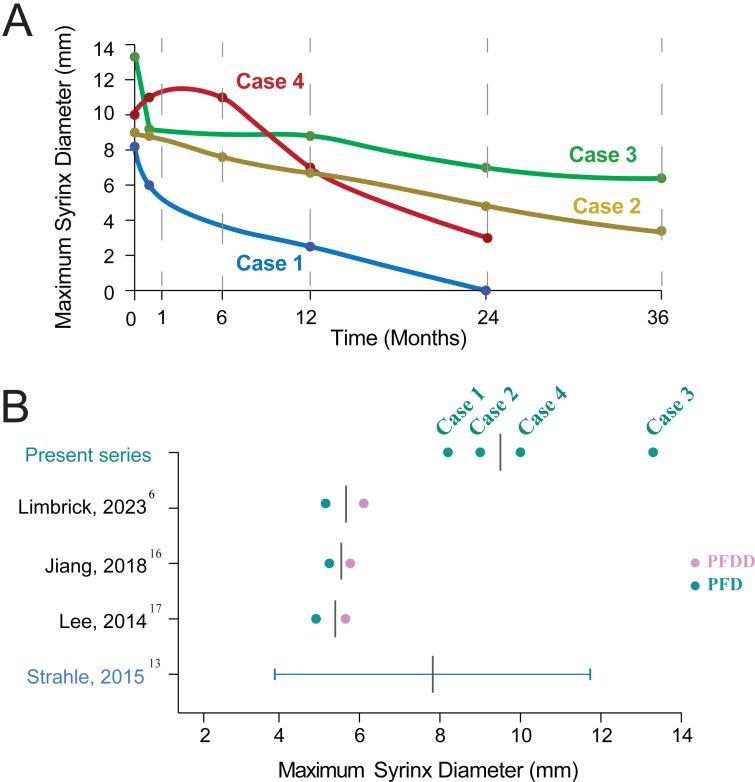
Observations: In a proof-of-principle study, the authors prospectively included 4 patients with CM-I, aged 3-15 years, with severe symptomatic syringes (spanning multiple cervical/thoracic levels and/or focally expanding the spinal cord) to undergo PFD with pre- and postdissection intraoperative MRI (iMRI). In all cases, same-day postdissection iMRI cine images showed enhanced CSF flow compared with predissection iMRI findings. Three of the 4 patients showed early syrinx and symptom improvement (≤ 6 weeks); all showed improvements at long-term follow-up (≥ 2 years). The mean hospital length of stay (LOS) was 1.25 days, with no complications or repeat surgery needed, and the mean follow-up was 37.5 months.
Lessons: CM-I can be treated via PFD alone without duraplasty, even with a severe syrinx. Improved CSF flow is achieved intraoperatively, and the syrinx can significantly decrease over a 6-week to 1-year period postoperatively. Additional benefits include a low risk of complications and a short LOS. https://thejns.org/doi/10.3171/CASE24777.
Keywords: Chiari malformation type I; duraplasty; syringomyelia.
Figures
References
-
- Hankinson T Tubbs RS Wellons JC.. Duraplasty or not? An evidence-based review of the pediatric Chiari I malformation. Childs Nerv Syst. 2011;27(1):35-40. - PubMed
-
- Yahanda AT Limbrick DD Jr.. Posterior fossa decompression with or without duraplasty for Chiari I malformation. Neurosurg Clin N Am. 2023;34(1):105-111. - PubMed
-
- Durham SR Fjeld-Olenec K.. Comparison of posterior fossa decompression with and without duraplasty for the surgical treatment of Chiari malformation Type I in pediatric patients: a meta-analysis. J Neurosurg Pediatr. 2008;2(1):42-49. - PubMed
-
- Limonadi FM Selden NR.. Dura-splitting decompression of the craniocervical junction: reduced operative time, hospital stay, and cost with equivalent early outcome. J Neurosurg. 2004;101(2suppl):184-188. - PubMed
LinkOut - more resources
Full Text Sources
