

Immune evasion mechanisms in early-stage I high-grade serous ovarian carcinoma: insights into regulatory T cell dynamics
- PMID: 40164596
- PMCID: PMC11958665
- DOI: 10.1038/s41419-025-07557-5
Immune evasion mechanisms in early-stage I high-grade serous ovarian carcinoma: insights into regulatory T cell dynamics
Erratum in
-
Correction: Immune evasion mechanisms in early-stage I high-grade serous ovarian carcinoma: insights into regulatory T cell dynamics.Cell Death Dis. 2025 May 16;16(1):387. doi: 10.1038/s41419-025-07701-1. Cell Death Dis. 2025. PMID: 40379632 Free PMC article. No abstract available.
Abstract
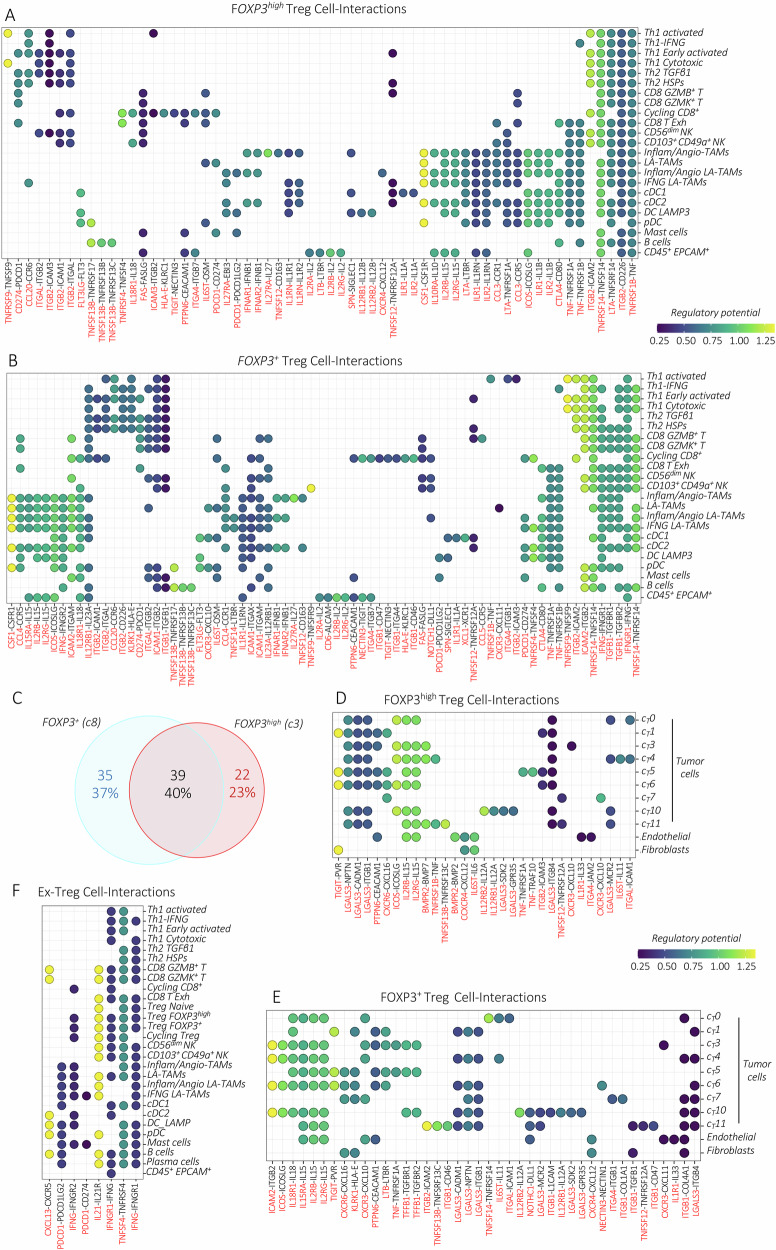
The mechanisms driving immune evasion in early-stage I high-grade serous ovarian carcinoma (HGSOC) remain poorly understood. To investigate this, we performed single-cell RNA-sequencing analysis. Our findings revealed a highly immunosuppressive HGSOC microenvironment, characterized by abundant infiltration of regulatory T cells (Tregs). Trajectory analysis uncovered differentiation pathways of naïve Tregs, which underwent either activation and proliferation or transcriptional instability. The predicted Treg-cell interaction network, including crosstalk within tumor cells, facilitates Treg mobility and maturation while reinforcing their immunosuppressive function and persistence in the tumor. Moreover, their interactions with immune cells likely inhibit CD8 T cells and antigen-presenting cells, supporting tumor immune escape. Additionally, more immunogenic tumor conditions, marked by IFNγ production, may contribute to Treg destabilization. Our findings underscore the pivotal role of Tregs in early immune evasion of HGSOC and provide insights into potential therapeutic strategies targeting their activity and differentiation fate.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures






References
-
- Zhang L, Conejo-Garcia JR, Katsaros D, Gimotty PA, Massobrio M, Regnani G, et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N Engl J Med. 2003;348:203–13. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Joyce JA, Fearon DT. T cell exclusion, immune privilege, and the tumor microenvironment. Science. 2015;348:74–80. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
