

Using human-centered design to advance health literacy in local health department programming: a case study
- PMID: 40165172
- PMCID: PMC11956235
- DOI: 10.1186/s12889-025-22491-z
Using human-centered design to advance health literacy in local health department programming: a case study
Abstract
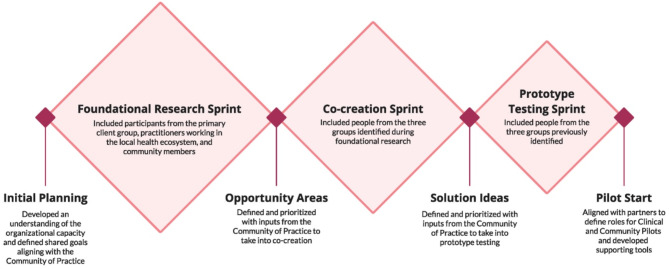
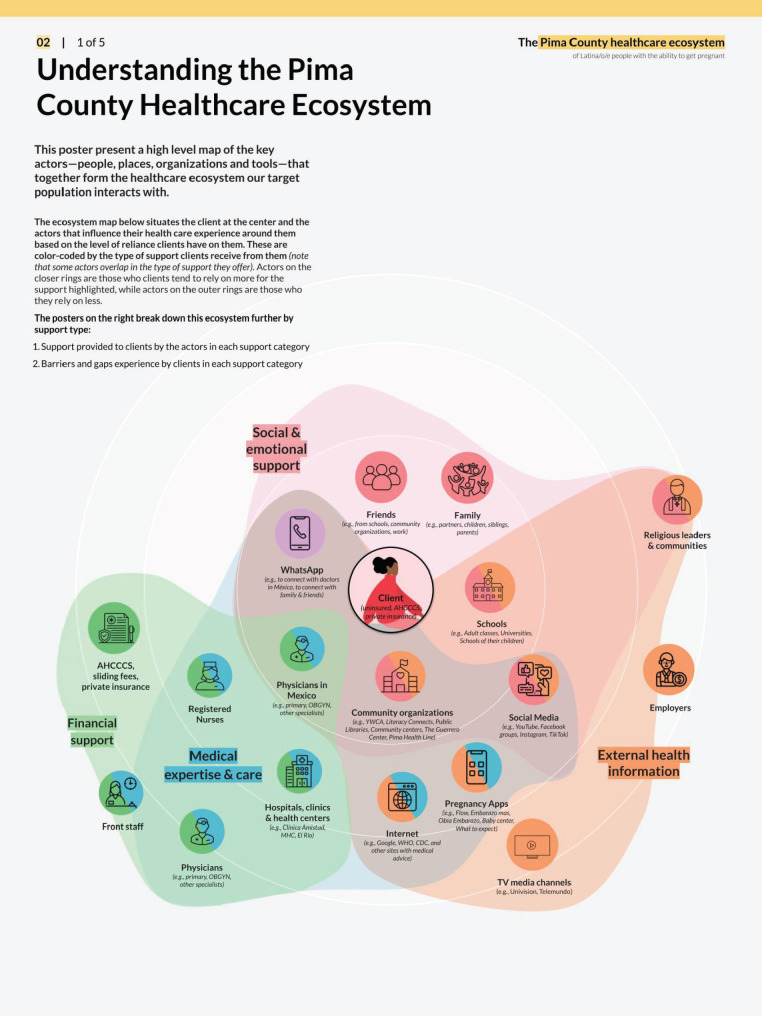
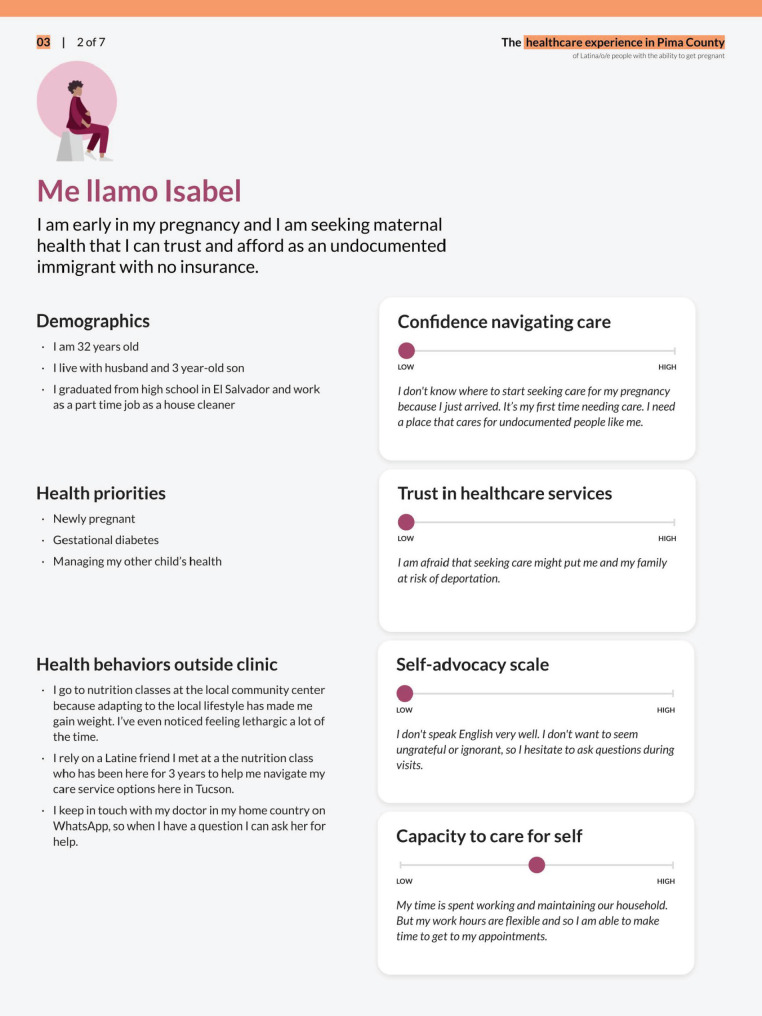
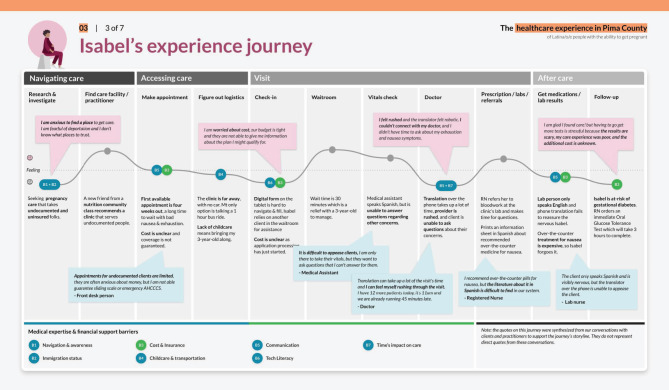
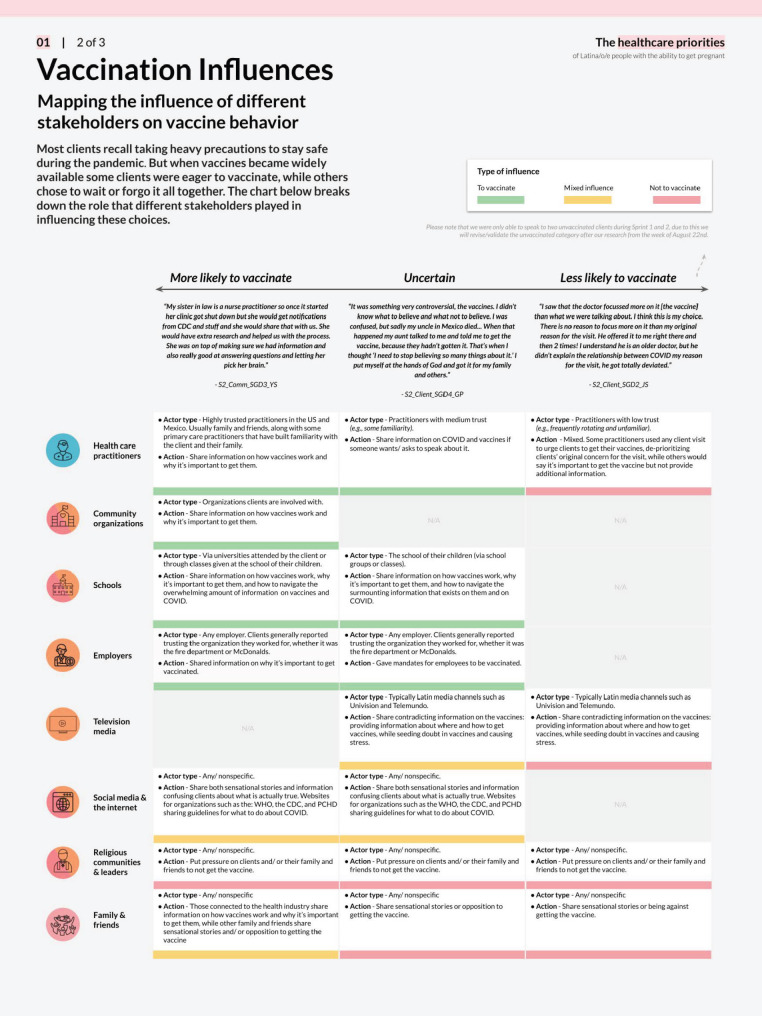
Background: Human-centered design (HCD) and behavioral science are structured, evidence-based methodologies used to develop and evaluate community-driven interventions. While HCD focuses on deeply understanding user needs and co-designing solutions, behavioral science applies empirically tested principles to drive behavior change. Together, these methodologies enable the development of interventions that are both user-centered and behaviorally informed. The Pima County Health Department and project partners leveraged these collaborative methodologies to assemble a Community of Practice to improve health literacy and adherence to COVID-19 public health practices among Hispanic/Latine individuals of childbearing age and ability in Pima County.
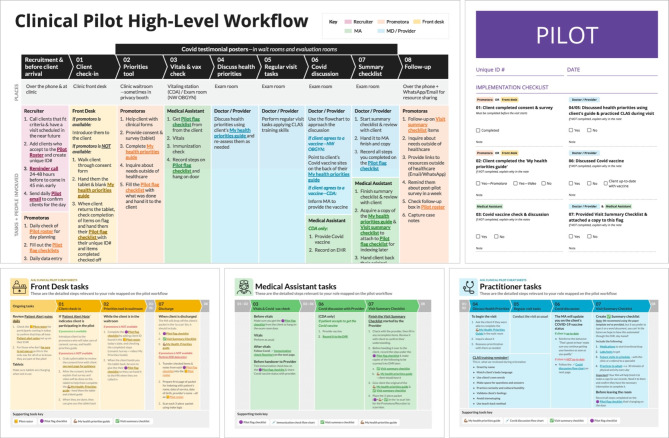
Methods: Human-centered design processes identified and evaluated barriers facing the target population. On the basis of these findings, two pilot interventions were implemented between July 2023 and November 2023: one in a clinical setting with 92 participants and another in a community setting with 207 participants. A mixed-methods approach was used to evaluate the impact of these pilots. Quantitatively, a pre-post evaluation and survey design estimated the effect of an intervention by comparing outcomes before and after implementation using paired t-test and chi-square tests. Qualitatively, structured post intervention interviews were conducted with participants who were randomly selected based upon their initial consent and willingness to participate.
Results: Participants in the clinical and community pilots perceived fewer barriers to health-seeking behaviors after the intervention. Both pilots increased participants' confidence in health-seeking behaviors (p < 0.01). Only the clinical pilot resulted in an increase in health literacy. In the clinical pilot, the number of unvaccinated participants decreased, and the number of participants who reported needing a booster increased. The community pilot did not find a statistically significant difference in COVID-19 vaccine uptake.
Conclusions: Integrating human-centered design and behavioral science into public health interventions can improve health literacy and confidence in health-seeking behaviors among historically and contemporarily excluded populations. Local health departments can use these methods to develop multicomponent interventions that foster mutual co-invention with communities and improve population health outcomes. Future research should focus on long-term impacts and explore broader applications of these approaches in different contexts.
Trial registration: This project received University of Arizona IRB review and approval. This study was not considered a randomized controlled trial and did not require registration.
Keywords: Community health workers; Equity; Health literacy; Human-centered design; Inclusion; Participatory design; Public health.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study adhered to the Helsinki Declaration and was approved by The University of Arizona Internal Review Board, Approval: STUDY00001990 before implementation. Due to the nature of the interventions applied, RCT registration was waived. The protocol for this study was thoroughly reviewed and approved by the University of Arizona Institutional Review Board (IRB), ensuring that it meets all ethical standards and guidelines as set forth by the board. The review process included an assessment of potential risks and benefits to participants, as well as the strategies put in place to minimize any risks. Informed consent is a cornerstone of our study. Prior to participation, all individuals were provided with comprehensive information about the study’s purpose, procedures, potential risks, and benefits. This information was communicated both verbally and through a written consent form. Participants were given ample opportunity to ask questions and consider their participation. The consent form used in this study, titled “MHC Healthcare: Consent to Participate in Research,” included detailed information about the study titled “Pima County: Advancing Health Literacy,” led by Principal Investigators Katrina Kelly (MHC Healthcare) and Dr. Ada Wilkinson-Lee (University of Arizona), and sponsored by the Centers for Disease Control and Prevention and the Pima County Health Department. Key elements of the consent form included: • A summary of the research, highlighting the study’s purpose to improve outreach and engagement with healthcare practitioners and Hispanic/Latine/Latinx individuals of childbearing age (20–45 years old) to increase vaccine confidence and coverage of COVID-19 vaccination. • A description of the major requirements of the study, including practitioner training, completion of pre- and post-surveys, participant engagement with promotoras, and optional participation in a 1-hour interview. • Information on the voluntary nature of participation, emphasizing that participants could withdraw at any time without any consequences. • Detailed explanations of the time commitment involved, potential risks and benefits, and the confidentiality measures in place to protect participant data. • Contact information for the Principal Investigators and the University of Arizona Institutional Review Board for participants to ask questions or raise concerns. To ensure comprehension, consent forms were written in clear, plain language, and were available in multiple languages to accommodate non-English speaking participants. All facilitators, practitioners, and staff who interacted with any program participants were required to take: Human Subjects Research (HSR) content is organized into two tracks: Biomedical (Biomed) and Social-Behavioral-Educational (SBE). Participants provided their consent by signing the consent form, and receiving a copy of the consent form, indicating their voluntary agreement to participate in the study. Participants were informed that their participation was voluntary and that they could withdraw from the study at any time without any consequences to their access to services or other benefits. Confidentiality of all personal information was maintained throughout the study, Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- US Office of Disease Prevention and Health Promotion. Health Literacy in Healthy People 2030. Healthy People 2030. US Department of Health and Human Services. https://health.gov/healthypeople/priority-areas/health-literacy-healthy-.... Accessed 1 Aug 2024.
-
- Brach C, Keller D, Hernandez LM, Baur C, Parker R, Dreyer B, Schyve P, Lemerise AJ, Schillinger D. Ten attributes of health literate health care organizations. NAM Perspect. 2012 Jun 19.
-
- Kutner M, Greenburg E, Jin Y, Paulsen C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy. NCES 2006– 483. National Center for education statistics. 2006 Sep.
-
- Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy to health outcomes. Am J Health Behav. 2007;31(1):S19–26. - PubMed
-
- Abbato S, Ryan J, Skelly C, Good P. The other side of getting by: a case study of interpreting provision decision-making and consequences for patients. Cogent Med. 2018;5(1):1483096.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
