

This is a preprint.
Combination immunotherapy induces post-intervention control of HIV
- PMID: 40166020
- PMCID: PMC11957202
- DOI: 10.21203/rs.3.rs-6141479/v1
Combination immunotherapy induces post-intervention control of HIV
Abstract
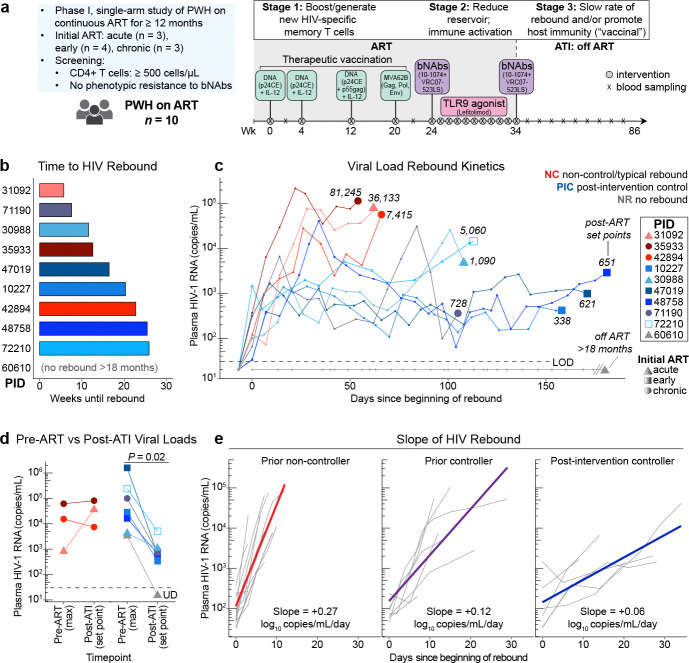
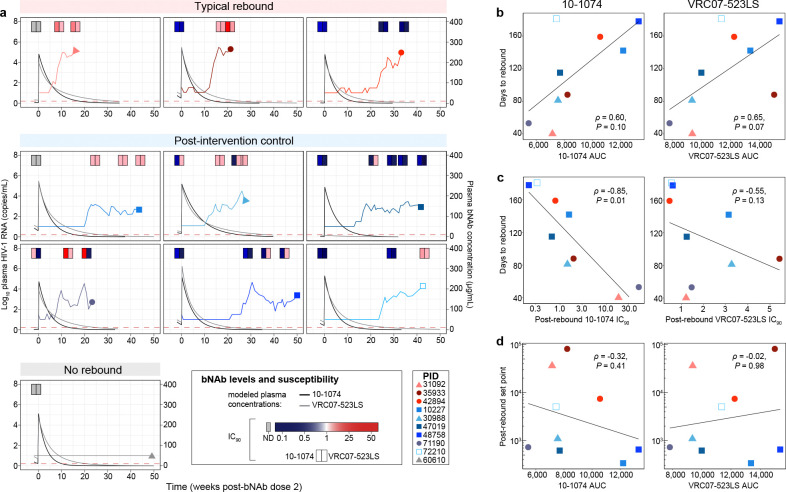
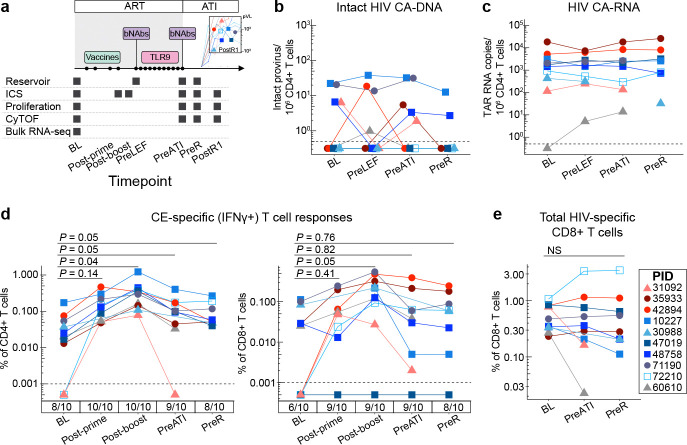
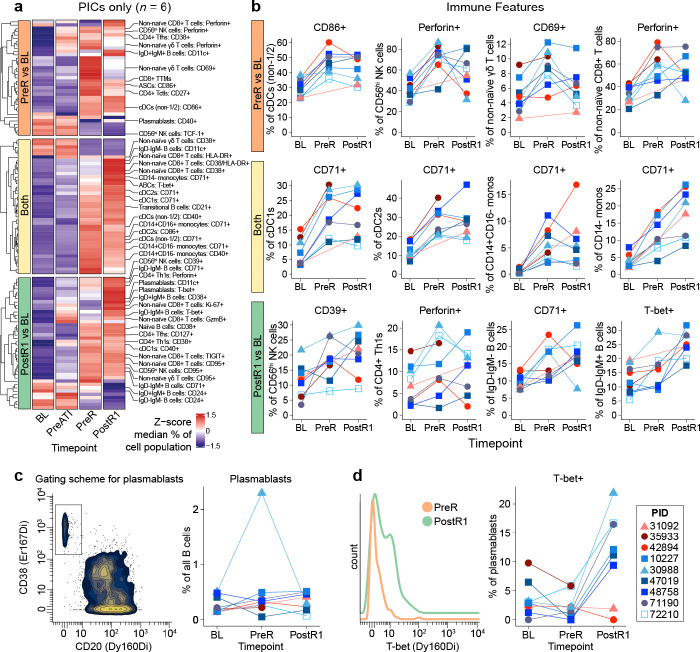
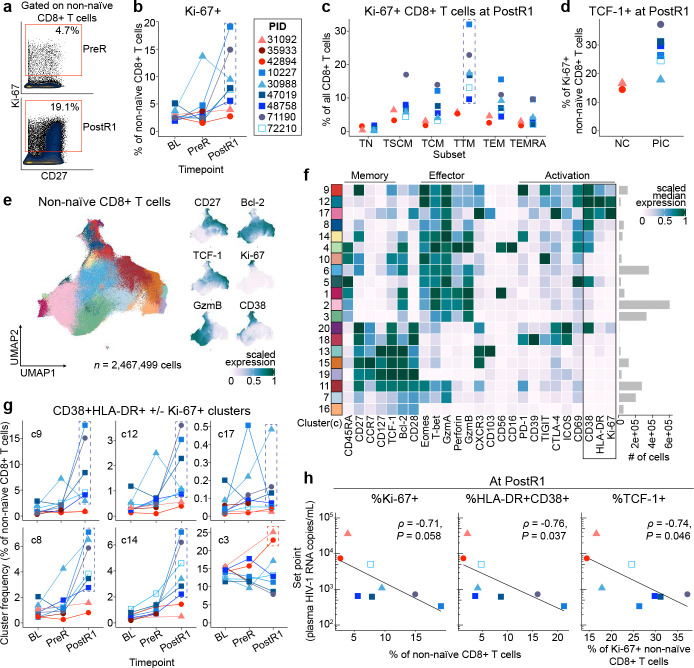
The identification of therapeutic strategies to induce sustained antiretroviral therapy (ART)-free control of HIV infection is a major priority.1 Combination immunotherapy including HIV vaccination, immune stimulation/latency reversal, and passive transfer of broadly neutralizing antibodies (bNAbs) has shown promise in non-human primate models,2-7 but few studies have translated such approaches into people. Here, we performed a single-arm, proof-of-concept combination study of these three approaches in ten people with HIV on ART that included (1) therapeutic vaccination with an HIV/Gag conserved element (CE)-targeted DNA+IL-12 prime/MVA boost regimen followed by (2) administration of two bNAbs (10-1074 and VRC07-523LS) and a toll-like receptor 9 (TLR9) agonist (lefitolimod) during ART suppression, followed by (3) repeat bNAb administration at the time of ART interruption. Seven of the ten participants exhibited partial (low viral load set point) or complete (aviremic) post-intervention control after stopping ART, independent of residual bNAb plasma levels. Robust expansion of activated CD8+ T cells early in response to rebounding virus correlated with lower viral load set points. These data suggest that combination immunotherapy approaches might prove effective to induce sustained control of HIV by slowing rebound and improving CD8+ T cell responses, and that these approaches should continue to be optimized.
Conflict of interest statement
Competing interest declaration MJP serves on a DSMB for American Gene Technologies. SGD reports consulting fees from AbbVie, Eli Lilly, Enanta, GSK, Hookipa, and Immunocore, participated on an advisory board for American Gene Technologies, and owns Tendel stock. MHS is founder and shareholder of Pro Biosciences and Teiko.bio, has been a paid consultant for Five Prime, Ono, January, Earli, Astellas, and Indaptus Therapeutics, and reports research funding from Roche/Genentech, Pfizer, Valitor, and Bristol Myers Squibb. MC served on a Gilead scientific advisory board. MCN has a patent to the bNAbs 10–1074 and 3BNC117 issued (Gilead), is on the SAB of Celldex, and reports personal fees from Gilead and Frontier Biosciences. BKF, GNP, and JIM are inventors on US Government-owned patents related to the CE DNA vaccine. MK has received funding to her institution from Gilead Sciences Inc and Intercept Pharmaceuticals and serves as a scientific consultant for Gilead Sciences Inc, GSK pharmaceuticals, and Resolution Therapeutics. JDR and CJP are employees of Labcorp-Monogram Biosciences and shareholders of Labcorp. DS and EV are employees of and hold stock in Gilead Sciences, Inc.
Figures
References
-
- Landovitz R. J., Scott H. & Deeks S. G. Prevention, treatment and cure of HIV infection. Nat. Rev. Microbiol. 21, 657–670 (2023). - PubMed
Publication types
Grants and funding
- R01 DE032033/DE/NIDCR NIH HHS/United States
- K23 AI162249/AI/NIAID NIH HHS/United States
- L30 AI147223/AI/NIAID NIH HHS/United States
- UM1 AI164560/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- INV-002707/GATES/Gates Foundation/United States
- R01 AI170239/AI/NIAID NIH HHS/United States
- P30 AI152501/AI/NIAID NIH HHS/United States
- P01 AI169606/AI/NIAID NIH HHS/United States
- T32 GM136547/GM/NIGMS NIH HHS/United States
- K23 AI157875/AI/NIAID NIH HHS/United States
- K24 AA022523/AA/NIAAA NIH HHS/United States
- UL1 TR001872/TR/NCATS NIH HHS/United States
- T32 AI060530/AI/NIAID NIH HHS/United States
- K24 AI174971/AI/NIAID NIH HHS/United States
- P01 AI178375/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
