

New insights into imaging of pulmonary metastases from extra-thoracic neoplasms
- PMID: 40167931
- PMCID: PMC12185656
- DOI: 10.1007/s11547-025-02008-9
New insights into imaging of pulmonary metastases from extra-thoracic neoplasms
Abstract
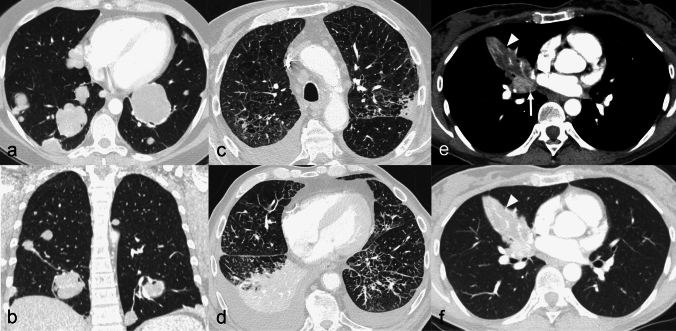
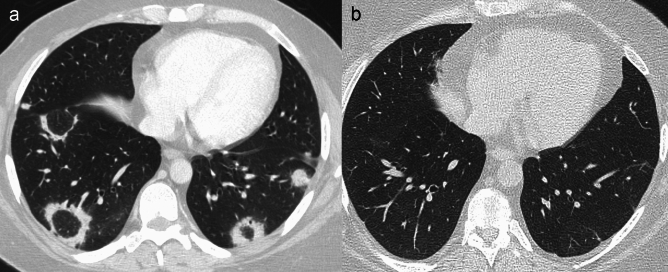
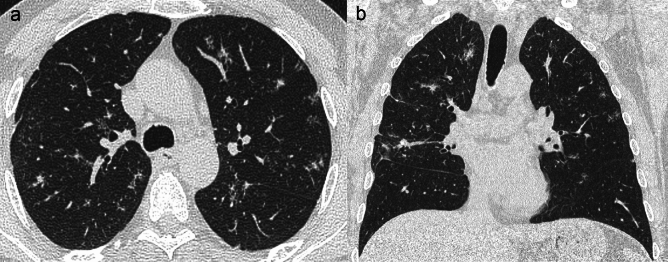
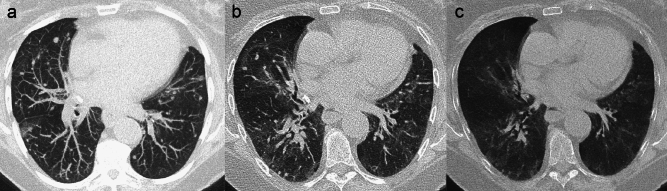
The lung is one of the most common sites of metastases from extra-thoracic neoplasms. Lung metastases can show heterogeneous imaging appearance, thus mimicking a wide range of lung diseases, from benign lesions to primary lung cancer. The proper interpretation of pulmonary findings is crucial for prognostic assessment and treatment planning, even to avoid unnecessary procedures and patient anxiety. For this purpose, computed tomography (CT) is one of the most used imaging modalities. In the last decades, cancer patients' population has steadily increased and, due to the widespread application of CT for staging and surveillance, the detection of pulmonary nodules has raised, making their characterization and management an urgent and mostly unsolved problem for both radiologists and clinicians. This review will highlight the pathways of dissemination of extra-thoracic tumours to the lungs and the heterogeneous CT imaging appearance of pulmonary metastases, providing useful clues to properly address the diagnosis. Furthermore, we will deal with the promising applications of radiomics in this field. Finally, a focus on the hot-topic of pulmonary nodule management in patients with extra-thoracic neoplasms (ETNs) will be discussed.
Keywords: Cancer; Differential diagnoses; Management; Metastasis; Multimodal imaging; Pulmonary nodules.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures

References
-
- Gould MK, Tang T, Liu I-LA et al (2015) Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med 192:1208–1214. 10.1164/rccm.201505-0990OC - PubMed
-
- Araujo-Filho JAB, Halpenny D, McQuade C et al (2021) Management of pulmonary nodules in oncologic patients: AJR expert panel narrative review. Am J Roentgenol 216:1423–1431. 10.2214/AJR.20.24907 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
