

Invasive Group A Streptococcal Infection in Children, 1992-2023
- PMID: 40168022
- PMCID: PMC11962665
- DOI: 10.1001/jamanetworkopen.2025.2861
Invasive Group A Streptococcal Infection in Children, 1992-2023
Abstract
Importance: The resurgence of invasive group A streptococcal (iGAS) infections and progress in GAS vaccine development emphasize the importance of understanding current trends in the epidemiology of iGAS.
Objective: To describe the epidemiology of pediatric iGAS over a 32-year period.
Design, setting, and participants: This case series uses population-based surveillance data for iGAS in Toronto and Peel Region, Canada, including emm typing from Canada's National Microbiology Laboratory and population data from Statistics Canada. All children (age <18 years) with iGAS from January 1, 1992, to December 31, 2023, were included. Data were analyzed from July 15, 2023, to September 1, 2024.
Main outcomes and measures: Outcomes of interest were disease incidence over time and by age; variation in clinical presentation, disease severity, outcomes and infecting emm types; and antimicrobial resistance.
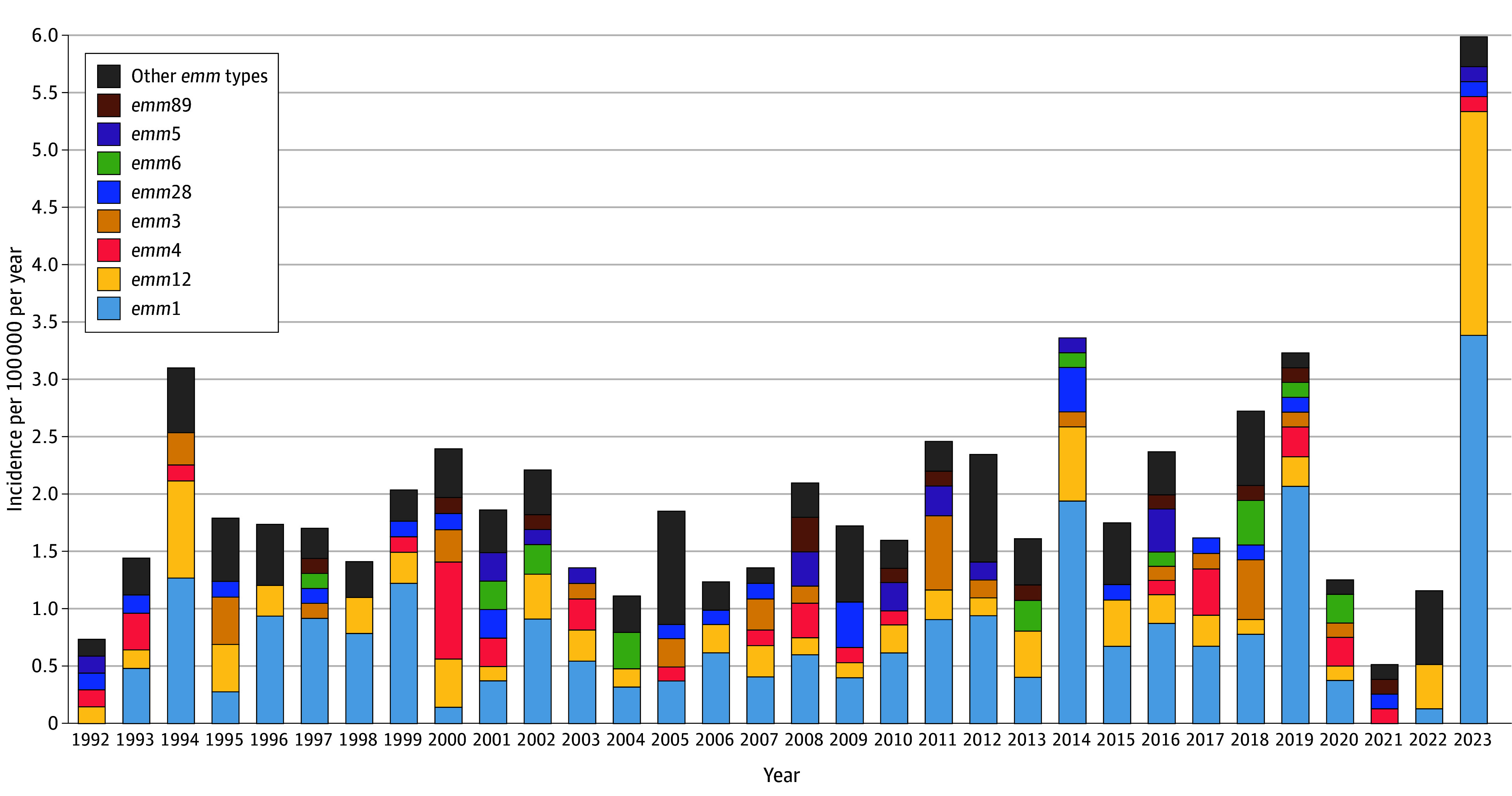
Results: Overall, 498 iGAS cases (300 [60.2%] male; median [IQR] age, 5.1 [2.7-8.6] years) occurred, including 151 (30.7%) in children with comorbidities. The most common presentations were soft tissue infection (140 cases [28.1%]) and bacteremia without focus (131 cases [26.3%]). iGAS incidence increased from 1.8 events per 100 000 population per year in 1992 to 2011 to 2.4 events per 100 000 population per year in 2012 to 2019 (incidence rate ratio, 1.3 [95% CI, 1.1-1.6]), with the increase occurring in GAS infections of the respiratory tract. Incidence declined to 1.2 events per 100 000 population per year in 2020 and 0.5 events per 100 000 population per year in 2021 before increasing to 6.0 events per 100 000 population per year in 2023. In 2022 to 2023, 18 of 56 children with iGAS (32.0%) had a viral respiratory coinfection. Varicella-associated iGAS cases declined from 23 of 137 children (16.8%) in 1992 to 2001 to 2 of 223 children (0.9%) in 2012 to 2023 (P < .001), after routine varicella vaccination implementation in 2004. Streptococcal toxic shock syndrome occurred in 29 children (5.8%), necrotizing fasciitis in 12 children (2.4%); 10 children (2.0%) died. The most common emm types were emm1 (182 of 471 isolates [38.6%]), emm12 (75 isolates [15.9%]), and emm4 (31 isolates [6.6%]). The M1UK subtype was first identified in 2019 and comprised 32 of 46 emm1 isolates (70.0%) from 2019 to 2023. Compared with other emm types, emm1 was more likely to be associated with pneumonia (odds ratio [OR], 1.99 [95% CI, 1.16-3.40]), bone and joint infections (OR, 1.70 [95% CI, 1.08-2.68]), and intensive care unit admission (OR, 1.67 [95% CI, 1.03-2.68]); emm4 was more likely to be associated with bacteremia without focus (OR, 6.10 [95% CI, 2.83-13.16]). Overall, 437 isolates (92.8%) were of emm types included in the 30-valent GAS vaccine.
Conclusions and relevance: This case series found that pediatric iGAS incidence increased in south-central Ontario prior to and after the COVID-19 pandemic in association with increased iGAS infections of the respiratory tract. Respiratory viral coinfections were common. Different emm types were associated with differing presentations and severity.
Conflict of interest statement
Figures


Comment in
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
