

A genotype-first approach identifies high incidence of NF1 pathogenic variants with distinct disease associations
- PMID: 40169570
- PMCID: PMC11962086
- DOI: 10.1038/s41467-025-57077-1
A genotype-first approach identifies high incidence of NF1 pathogenic variants with distinct disease associations
Abstract
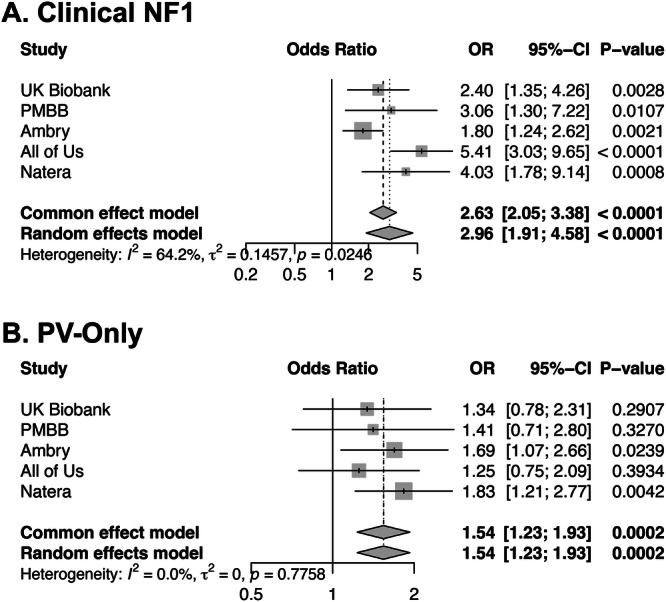
Loss of function variants in the NF1 gene cause neurofibromatosis type 1, a genetic disorder characterized by complete penetrance, characteristic physical exam findings, and a substantially increased risk for malignancy. However, our understanding of the disorder is based on patients ascertained through phenotype-first approaches, which estimate prevalence at 1 in 3000. Leveraging a genotype-first approach in multiple large patient cohorts including over one million individuals, we demonstrate an unexpectedly high prevalence (1 in 1,286) of NF1 pathogenic variants. Half are identified in individuals lacking clinical features of NF1, with many appearing to have post-zygotic mosaicism for the identified variant. Incidentally discovered variants are not associated with classic neurofibromatosis features but are associated with an increased incidence of malignancy compared to control populations. Our findings suggest that NF1 pathogenic variants are substantially more common than previously thought, often characterized by somatic mosaicism and reduced penetrance, and are important contributors to cancer risk in the general population.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: E.C., C.H., J.S.D., A.Y., M.R., V.S., and S.L. are employees of Ambry Genetics. K.L., J.Z., C.B.S., A.E., and Y.S. are employees of Natera Inc. J.W. is a consultant for Natera Inc. The authors declare no other competing interests.
Figures




Update of
-
A genotype-first approach identifies high incidence of NF1 pathogenic variants with distinct disease associations.medRxiv [Preprint]. 2023 Aug 10:2023.08.08.23293676. doi: 10.1101/2023.08.08.23293676. medRxiv. 2023. Update in: Nat Commun. 2025 Apr 01;16(1):3121. doi: 10.1038/s41467-025-57077-1. PMID: 37609227 Free PMC article. Updated. Preprint.
References
-
- Karaconji, T., Whist, E., Jamieson, R. V., Flaherty, M. P. & Grigg, J. R. B. Neurofibromatosis type 1: review and update on emerging therapies. Asia Pac. J. Ophthalmol.8, 62–72 (2019). - PubMed
-
- Stewart, D. R., Korf, B. R., Nathanson, K. L., Stevenson, D. A. & Yohay, K. Care of adults with neurofibromatosis type 1: a clinical practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet. Med.20, 671–682 (2018). - PubMed
-
- Evans, D. G. et al. Birth incidence and prevalence of tumor-prone syndromes: estimates from a UK family genetic register service. Am. J. Med. Genet. A152A, 327–332 (2010). - PubMed
MeSH terms
Substances
Grants and funding
- T32 GM008638/GM/NIGMS NIH HHS/United States
- P50 GM115318/GM/NIGMS NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- U2C OD023196/OD/NIH HHS/United States
- OT2 OD026551/OD/NIH HHS/United States
- U24 OD023121/OD/NIH HHS/United States
- OT2 OD026552/OD/NIH HHS/United States
- OT2 OD026549/OD/NIH HHS/United States
- OT2 OD025337/OD/NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- OT2 OD025277/OD/NIH HHS/United States
- OT2 OD026555/OD/NIH HHS/United States
- OT2 OD026553/OD/NIH HHS/United States
- OT2 OD023205/OD/NIH HHS/United States
- OT2 OD026557/OD/NIH HHS/United States
- OT2 OD026554/OD/NIH HHS/United States
- OT2 OD023206/OD/NIH HHS/United States
- R01 CA176785/CA/NCI NIH HHS/United States
- OT2 OD026556/OD/NIH HHS/United States
- U24 OD023176/OD/NIH HHS/United States
- R01 AI077505/AI/NIAID NIH HHS/United States
- OT2 OD026548/OD/NIH HHS/United States
- K08 DK127247/DK/NIDDK NIH HHS/United States
- OT2 OD025315/OD/NIH HHS/United States
- OT2 OD026550/OD/NIH HHS/United States
- R01 AI116794/AI/NIAID NIH HHS/United States
- T32 HG008961/HG/NHGRI NIH HHS/United States
- OT2 OD025276/OD/NIH HHS/United States
- U24 OD023163/OD/NIH HHS/United States
- R01 CA192393/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
