

Red blood cell transfusion strategy in traumatic brain injury patients: a systematic review and meta-analysis
- PMID: 40170107
- PMCID: PMC11959887
- DOI: 10.1186/s40001-025-02498-3
Red blood cell transfusion strategy in traumatic brain injury patients: a systematic review and meta-analysis
Abstract
Background: The optimal red blood cell transfusion (RBCT) strategy for traumatic brain injury (TBI) patients remains a topic of debate. This systematic review and meta-analysis aimed to compare the outcomes of a liberal transfusion strategy versus a restrictive strategy in critically ill patients with TBI.
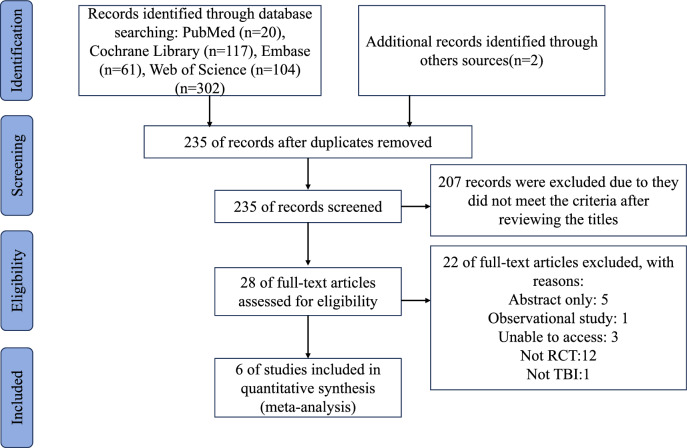
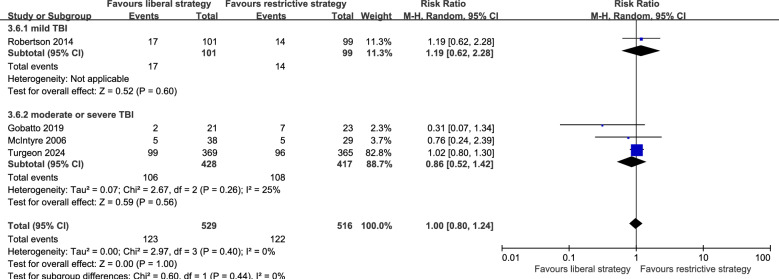
Methods: PubMed, Web of Science, Embase, and Cochrane Library were searched from inception to November 17, 2024. We included randomized controlled trials (RCTs) of critically ill adult patients with TBI, reporting data on RBCT strategies. The outcomes included intensive care unit (ICU) mortality, long-term mortality, unfavorable functional outcomes, and the incidence of adverse events, such as transfused acute respiratory distress syndrome (TARDS) and venous thromboembolism. We also performed subgroup analyses comparing the association between disease severity and long-term mortality. This review was submitted to PROSPERO (Registration number: CRD42024558797).
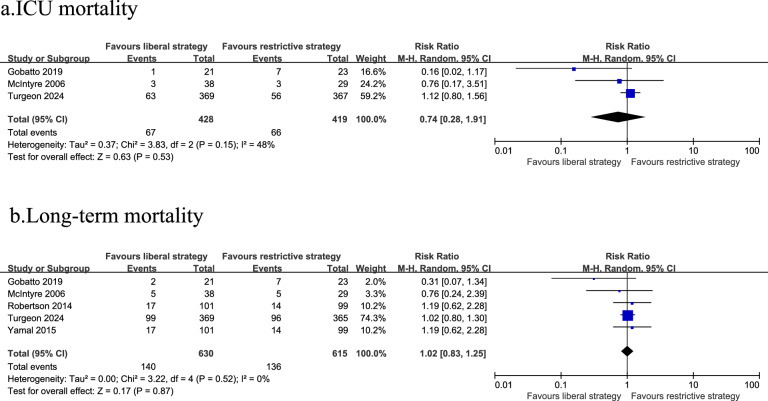
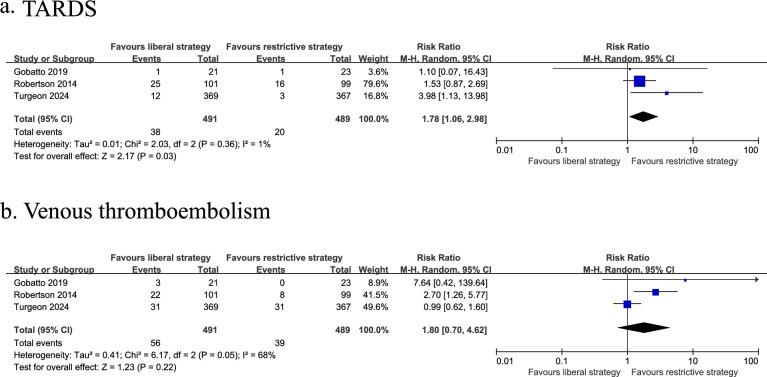
Results: In the results, our analysis revealed that compared to a restrictive transfusion strategy, a liberal strategy did not significantly reduce the risk of ICU mortality (RR: 0.74; 95% CI 0.28-1.91; P = 0.53) and long-term mortality (RR: 1.02; 95% CI 0.83-1.25; P = 0.87), but it was able to reduce the risk of unfavorable functional outcomes (RR: 0.90; 95% CI 0.82-0.98; P = 0.01), although there may be a false positive error. In addition, the liberal transfusion strategy was associated with a higher incidence of Transfused Acute Respiratory Distress Syndrome (TARDS) (RR: 1.78; 95% CI 1.06-2.98; P = 0.03).
Conclusions: In critically ill patients with TBI, a liberal RBCT strategy appears to improve functional outcomes but carries the risk of false positive errors. In addition, this strategy does not seem to improve survival and may increase the risk of TARDS. Despite this, there remains insufficient evidence to recommend either strategy in this population.
Keywords: Meta-analysis; Mortality; Red blood cell transfusion; Transfused acute respiratory distress syndrome; Traumatic brain injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support.Cochrane Database Syst Rev. 2017 Jan 27;1(1):CD011305. doi: 10.1002/14651858.CD011305.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2024 May 23;5:CD011305. doi: 10.1002/14651858.CD011305.pub3. PMID: 28128441 Free PMC article. Updated.
-
Transfusion thresholds for guiding red blood cell transfusion.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD002042. doi: 10.1002/14651858.CD002042.pub5. Cochrane Database Syst Rev. 2021. PMID: 34932836 Free PMC article.
-
Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support.Cochrane Database Syst Rev. 2024 May 23;5(5):CD011305. doi: 10.1002/14651858.CD011305.pub3. Cochrane Database Syst Rev. 2024. PMID: 38780066 Free PMC article.
-
Red blood cell transfusion for people undergoing hip fracture surgery.Cochrane Database Syst Rev. 2015 Apr 21;2015(4):CD009699. doi: 10.1002/14651858.CD009699.pub2. Cochrane Database Syst Rev. 2015. PMID: 25897628 Free PMC article.
-
Red blood cell transfusion management for people undergoing cardiac surgery for congenital heart disease.Cochrane Database Syst Rev. 2025 Mar 19;3(3):CD009752. doi: 10.1002/14651858.CD009752.pub3. Cochrane Database Syst Rev. 2025. PMID: 40105353
References
-
- Maas AIR, Menon DK, Adelson PD, Andelic N, Bell MJ, Belli A, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16:987–1048. - PubMed
-
- Gouvêa Bogossian E, Rass V, Lindner A, Iaquaniello C, Miroz JP, Cavalcante Dos Santos E, et al. Factors associated with brain tissue oxygenation changes after RBC transfusion in acute brain injury patients. Crit Care Med. 2022;50:e539-47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
