

The current use of vasoactive agents in cardiogenic shock related to myocardial infarction and acute decompensated heart failure
- PMID: 40170689
- PMCID: PMC11960524
- DOI: 10.1016/j.ahjo.2025.100524
The current use of vasoactive agents in cardiogenic shock related to myocardial infarction and acute decompensated heart failure
Abstract
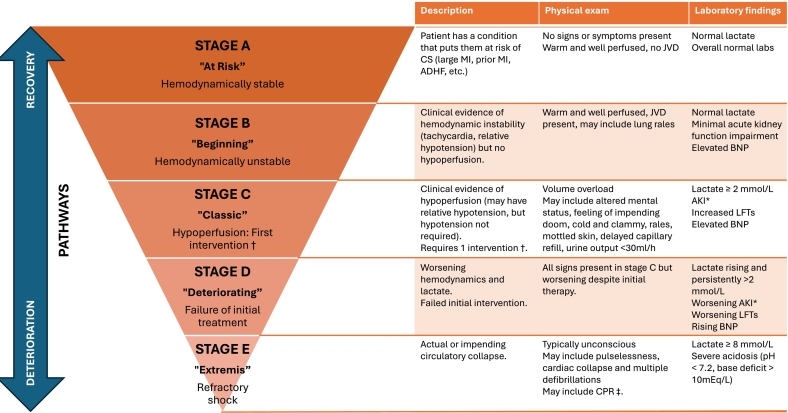
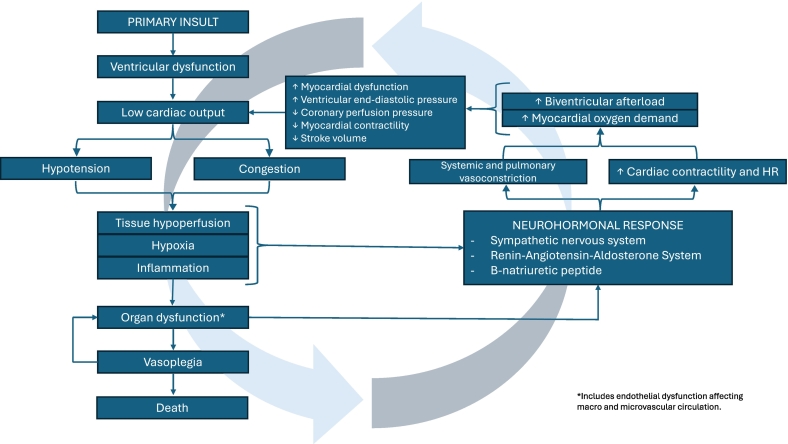
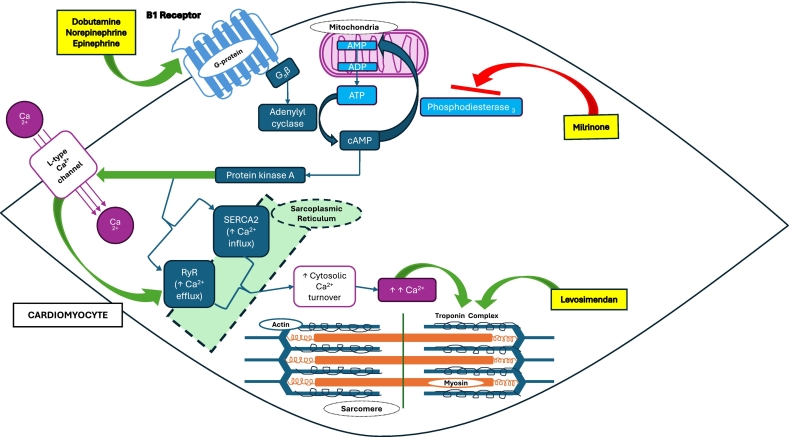
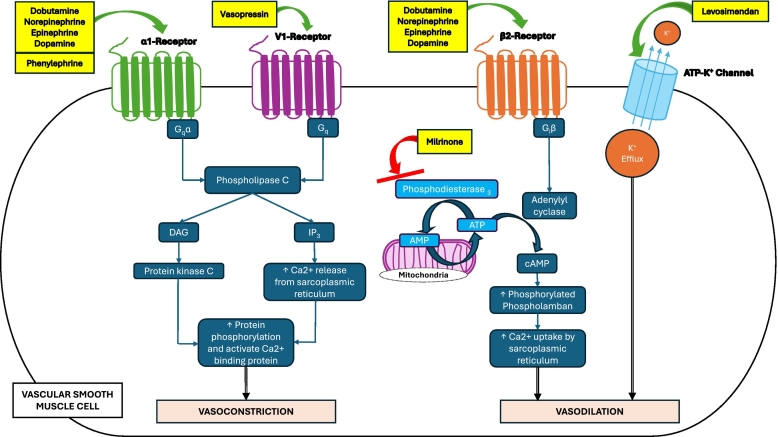
Cardiogenic shock (CS) is a heterogeneous condition associated with exceptionally high mortality rates, despite significant advances in the field of cardiology. The primary causes of CS are myocardial infarction-related CS (AMI-CS) and acute decompensated heart failure-related CS (ADHF-CS). Management of CS is inherently complex, with the initial focus-irrespective of the underlying etiology-centered on preserving end-organ perfusion. Parenteral vasopressors and inotropes are the cornerstone of therapy to achieve this objective. However, data on the comparative efficacy of different vasoactive agents in CS remain limited, and no single agent has demonstrated clear superiority. Recent progress in the staging and phenotyping of CS has provided a framework for more tailored therapeutic approaches. This review offers a comprehensive and updated summary of current evidence on the use of vasopressors and inotropes in AMI-CS and ADHF-CS, including a discussion of specific scenarios, such as right ventricular CS (RV-CS).
Keywords: Acute decompensated heart failure cardiogenic shock (ADHF-CS); Acute myocardial infarction cardiogenic shock (AMI-CS); Cardiogenic shock; Inotropes; Vasopressors.
© 2025 The Authors. Published by Elsevier Inc.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Differences between cardiogenic shock related to acute decompensated heart failure and acute myocardial infarction.ESC Heart Fail. 2023 Dec;10(6):3472-3482. doi: 10.1002/ehf2.14510. Epub 2023 Sep 18. ESC Heart Fail. 2023. PMID: 37723131 Free PMC article.
-
Comparison of the Hemodynamic Response to Intra-Aortic Balloon Counterpulsation in Patients With Cardiogenic Shock Resulting from Acute Myocardial Infarction Versus Acute Decompensated Heart Failure.Am J Cardiol. 2019 Dec 15;124(12):1947-1953. doi: 10.1016/j.amjcard.2019.09.016. Epub 2019 Sep 26. Am J Cardiol. 2019. PMID: 31648782 Free PMC article.
-
Improved mortality and haemodynamics with milrinone in cardiogenic shock due to acute decompensated heart failure.ESC Heart Fail. 2023 Aug;10(4):2577-2587. doi: 10.1002/ehf2.14379. Epub 2023 Jun 15. ESC Heart Fail. 2023. PMID: 37322827 Free PMC article.
-
Tailoring Pharmacological Treatment in Cardiogenic Shock: A Narrative Review.Discov Med. 2025 Feb;37(193):222-243. doi: 10.24976/Discov.Med.202537193.19. Discov Med. 2025. PMID: 39973548 Review.
-
Inotropic Agents and Vasopressors in the Treatment of Cardiogenic Shock.Curr Heart Fail Rep. 2020 Dec;17(6):438-448. doi: 10.1007/s11897-020-00493-9. Epub 2020 Oct 26. Curr Heart Fail Rep. 2020. PMID: 33103204 Review.
Cited by
-
Cardiogenic shock 2025: Understanding real world outcomes and contemporary practice to help guide improvements in care.Am Heart J Plus. 2025 May 20;55:100553. doi: 10.1016/j.ahjo.2025.100553. eCollection 2025 Jul. Am Heart J Plus. 2025. PMID: 40551756 Free PMC article. No abstract available.
References
-
- Hochman J.S., Sleeper L.A., Webb J.G., Sanborn T.A., White H.D., Talley J.D., Buller C.E., Jacobs A.K., Slater J.N., Col J., McKinlay S.M., LeJemtel T.H. Early revascularization in acute myocardial infarction complicated by cardiogenic SHOCK. SHOCK Investigators. Should we emergently Revascularize occluded coronaries for cardiogenic shock. N. Engl. J. Med. 1999;341(9):625–634. doi: 10.1056/NEJM199908263410901. Aug 26. (PMID: 10460813) - DOI - PubMed
-
- -Helgestad OKL, Josiassen J, Hassager C, Jensen LO, Holmvang L, Sørensen A, Frydland M, Lassen AT, Udesen NLJ, Schmidt H, Ravn HB, Møller JE. Temporal trends in incidence and patient characteristics in cardiogenic shock following acute myocardial infarction from 2010 to 2017: a Danish cohort study. Eur. J. Heart Fail. 2019 Nov;21(11):1370–1378. doi: 10.1002/ejhf.1566. Epub 2019 Jul 24. PMID: 31339222. - DOI - PubMed
-
- -van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, Thiele H, Washam JB, Cohen MG; American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Mission: Lifeline. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017 Oct 17;136(16):e232-e268. doi: 10.1161/CIR.0000000000000525. Epub 2017 Sep 18. PMID: 28923988. - DOI - PubMed
-
- -Osman *Khan MZ, Munir MB, Khan MU, Osman M, Agrawal P, Syed M, Ghaffar YA, Alharbi A, Khan SU, Balla S. Trends, Outcomes, and Predictors of Revascularization in Cardiogenic Shock. Am. J. Cardiol. 2020 Feb 1;125(3):328–335. doi: 10.1016/j.amjcard.2019.10.040. (Epub 2019 Nov 6. PMID: 31784052; PMCID: PMC7453955). - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
