

Robotic versus laparoscopic colectomy for transverse colon cancer: a systematic review and meta-analysis
- PMID: 40172685
- PMCID: PMC11965196
- DOI: 10.1007/s00384-025-04859-0
Robotic versus laparoscopic colectomy for transverse colon cancer: a systematic review and meta-analysis
Abstract
Purpose: Transverse colon cancer, which accounts for approximately 10% of all colon cancers, has a significant gap in the available scientific literature regarding the optimal minimally invasive surgical approach. This meta-analysis aims to compare the robotic and laparoscopic approaches for the surgical management of transverse colon cancer.
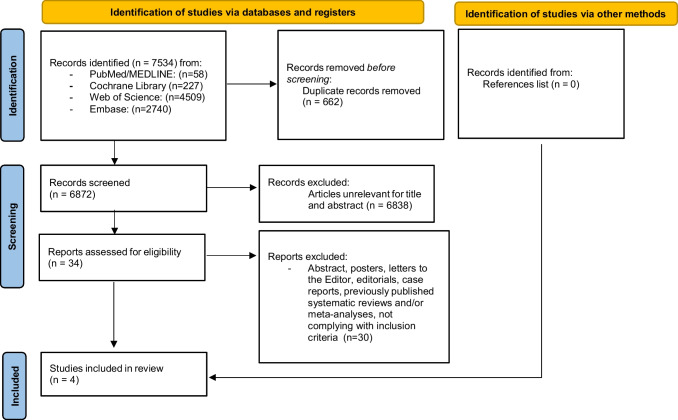
Methods: Our systematic review made use of Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines, in addition to Cochrane Handbook for Systematic Reviews of Interventions. Articles of interest turned out from a search with PubMed/MEDLINE, Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials-CENTRAL), Web of Science (Science and Social Science Citation Index), and Embase databases. A comprehensive literature search was conducted for comparative population studies concerning patients who underwent robotic or laparoscopic colectomy for transverse colon cancer). The risk of bias was assessed by the Cochrane Risk-of-Bias tool for randomized trials (Version 2) (RoB 2) and the Risk Of Bias In Non-randomized Studies - of Interventions (Version 2) ROBINS-I. We evaluated two groups of outcomes: intraoperative and postoperative. RevMan (Computer program) Version 5.4.1 was used to perform the meta-analysis. The heterogeneity of the included studies in the meta-analysis was assessed by using the I2 statist.
Results: The 4 included comparative studies (373 patients: 116 robotic colectomy versus 257 laparoscopic colectomy) had a time frame of approximately 26 years (2005-2021) and an observational nature. Meta-analysis showed a longer operative time (MD: 62.47, 95% CI: 18.17, 106.76, I2 = 92%, P = 0.006) and a shorter hospital stay (MD:-1.11, 95% CI: -2.05, -0.18, I2 = 63%, P = 0.002) for the robotic group. No differences in terms of conversion to laparotomy, estimated blood loss, time to flatus, time to solid diet, overall postoperative complications rate, minor (Clavien-Dindo or CD I-II) and major (Clavien-Dindo or CD ≥ III) postoperative complications rate, anastomotic leakage, surgical site infections, bleeding, lymph nodes harvested, were shown between robotic and laparoscopic groups.
Conclusions: Our meta-analysis revealed that the robotic approach to transverse colon cancer appears to be a safe and feasible option, with results comparable to those of laparoscopic surgery, with longer operating times but a shorter hospital stay. Further high-quality methodological studies are needed to evaluate and compare the short- and long-term outcomes, healthcare costs, and the learning curve between the robotic and laparoscopic surgical approaches.
Keywords: Extendend colectomy; Laparoscopic surgery; Robotic surgery; Segmental colectomy; Transverse colon cancer.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Statement of ethics: As our systematic review is based on previously published studies without any addition to original patient population data, approval by the Ethics Committee and informed patient consent were not required. Informed consent: Not applicable. Competing interests: The authors declare no competing interests. Institutional review board statement: Local ethics committee (Comitato Etico dell’Area Vasta Emilia Nord, Italy) ruled that no formal ethics approval was required in this study.
Figures














References
-
- Allemani C, Matsuda T, Di Carlo V et al (2018) Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391:1023–1075. 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
