

Radiotherapy Utilization in Traditional Medicare and Medicare Advantage
- PMID: 40172887
- PMCID: PMC11966333
- DOI: 10.1001/jamanetworkopen.2025.3018
Radiotherapy Utilization in Traditional Medicare and Medicare Advantage
Abstract
Importance: As more than 50% of Medicare beneficiaries are enrolled in Medicare Advantage (MA), understanding whether the treatment covered by MA vs traditional Medicare (TM) is comparable can aid in providing high-value care. As the majority of patients with cancer undergo radiotherapy, it is important to quantify TM and MA utilization in oncology.
Objective: To analyze the primary type of radiotherapy technology used, treatment length, and estimated spending for MA patients with cancer undergoing radiotherapy compared with TM patients with cancer.
Design, setting, and participants: This retrospective cross-sectional study used 2018 Medicare claims data for TM and MA patients aged 65 years or older who received radiotherapy for 1 of 15 cancer types. Analyses were performed between May 1 and December 28, 2024.
Exposures: Insurance type (MA vs TM), cancer type, age, dual-eligibility status, medical comorbidities, county, and radiotherapy center type.
Main outcomes and measures: Primary type of radiotherapy technology used, treatment length, and estimated spending for 90-day radiotherapy episodes. Adjusted rates and odds ratios (ORs) were calculated to compare technology types and rate ratios (RRs) to compare treatment length and estimated spending between TM and MA episodes.
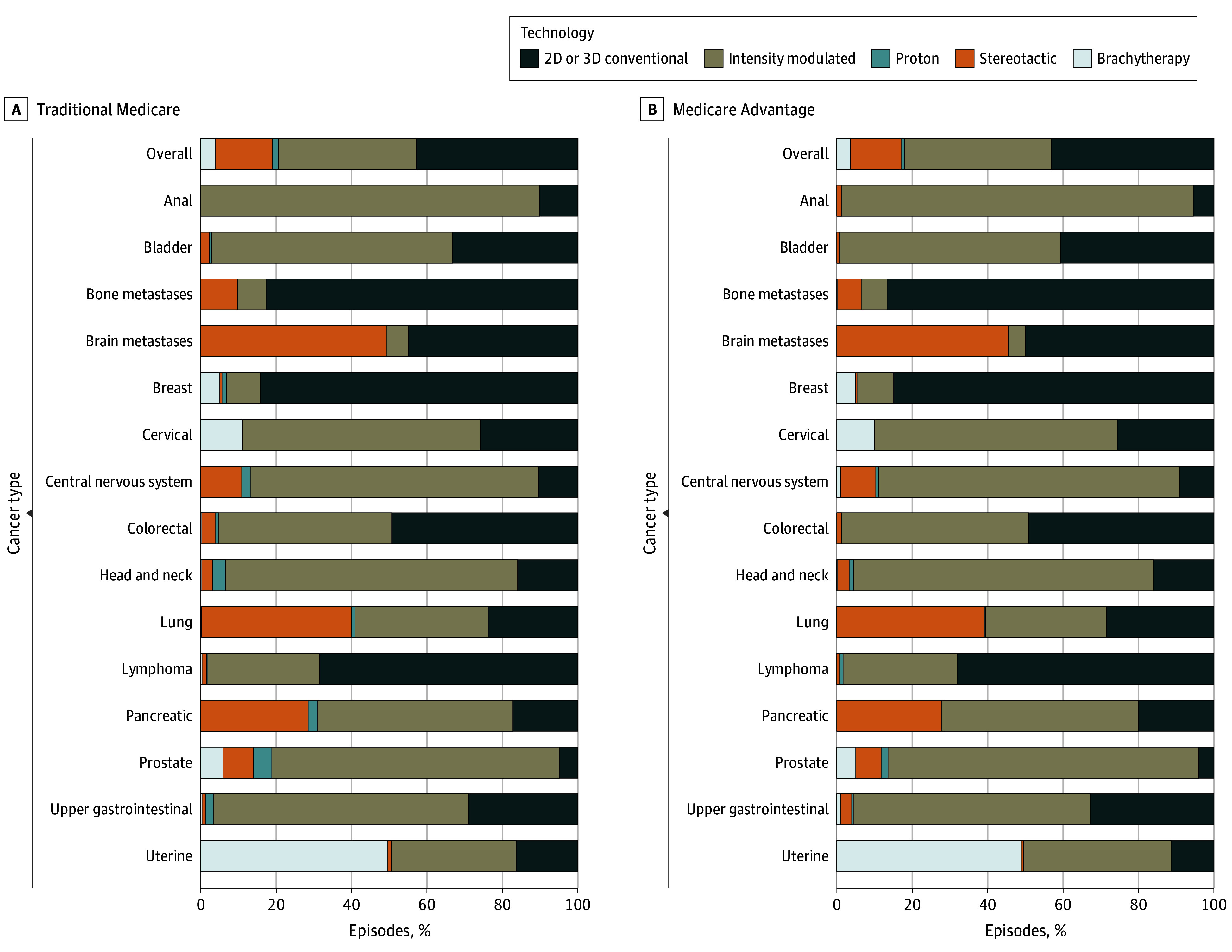
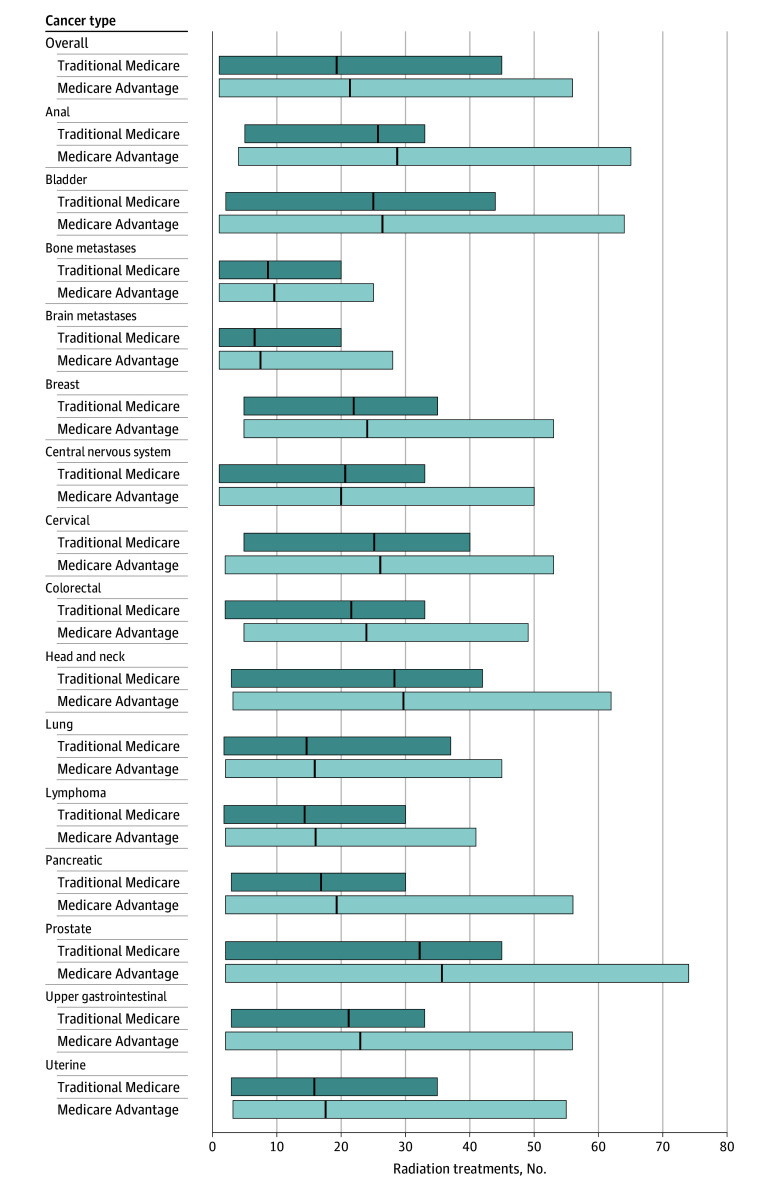
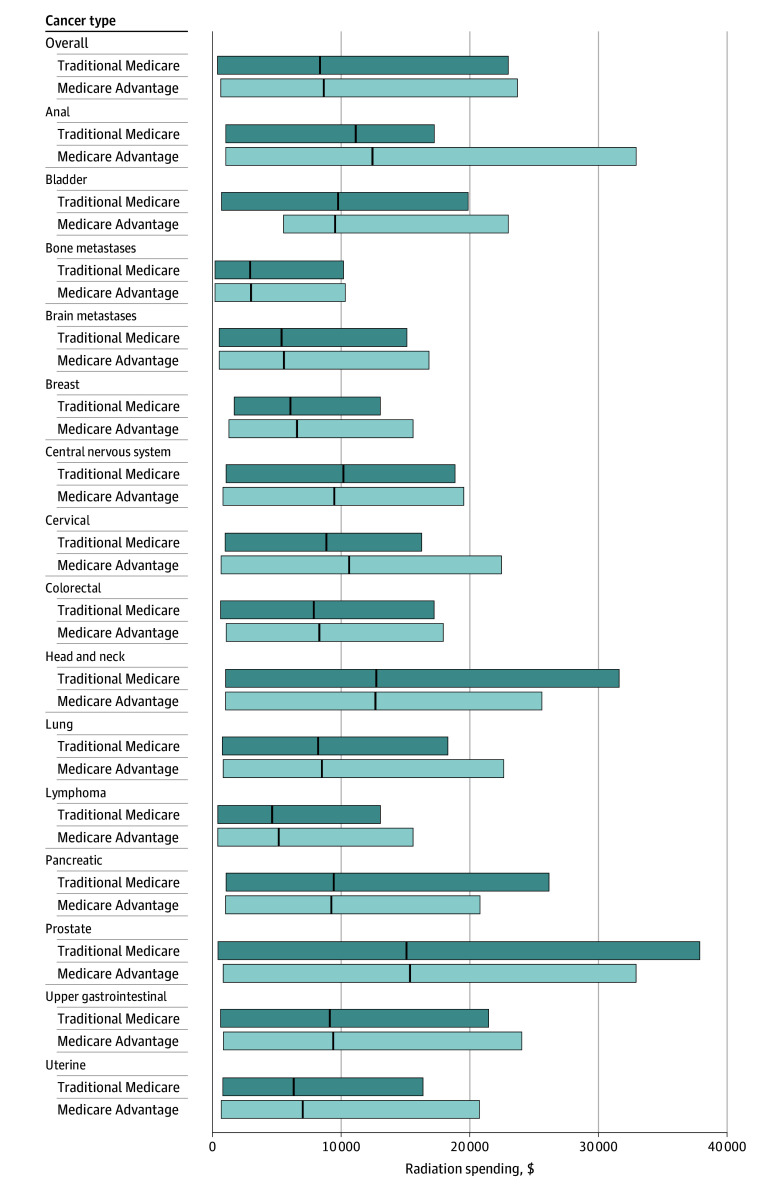
Results: Of 31 563 treatment episodes among 30 941 patients, 22 594 (71.58%) were covered by TM (mean [SD] age, 74.76 [6.57] years; 50.76% among males) and 8969 (28.42%) were covered by MA (mean [SD] age, 74.51 [6.24] years; 51.78% among males). For radiotherapy episodes in patients with MA, adjusted analyses revealed lower odds of proton therapy use (52 [0.58% (95% CI, 0.34%-0.82%)] vs 373 [1.65% (95% CI, 1.50%-1.80%)]; OR, 0.36 [95% CI, 0.27-0.48]) and stereotactic radiotherapy use (1235 [13.77% (95% CI, 13.13%-14.41%)] vs 3391 [15.01% (95% CI, 14.61%-15.41%)]; OR, 0.87 [95% CI, 0.81-0.95]), higher odds of 2- or 3-dimensional radiotherapy use (3962 [44.17% (95% CI, 43.39%-44.96%)] vs 9584 [42.43% (95% CI, 41.93%-42.92%)]; OR, 1.13 [95% CI, 1.06-1.21]), greater mean treatment length (21.38 [95% CI, 21.14-21.61] vs 19.48 [95% CI, 19.33-19.62] treatments; RR, 1.10 [95% CI, 1.08-1.11]), and higher estimated radiotherapy spending ($8677.56 [95% CI, $8566.58-$8788.54] vs $8393.20 [95% CI, $8323.34-$8463.05]; RR, 1.04 [95% CI, 1.02-1.06]) compared with episodes in patients with TM.
Conclusions and relevance: In this cross-sectional study, MA patients with cancer undergoing radiotherapy had higher estimated spending and greater mean treatment length than those covered by TM. Despite lower utilization of more expensive advanced treatment modalities, MA was not associated with cost savings. Whether MA meets the value proposition for radiation oncology requires further investigation.
Conflict of interest statement
Figures
Similar articles
-
Perioperative Costs of Elective Surgical Procedures in Medicare Advantage Compared With Traditional Medicare.JAMA Health Forum. 2025 Aug 1;6(8):e252258. doi: 10.1001/jamahealthforum.2025.2258. JAMA Health Forum. 2025. PMID: 40748544 Free PMC article.
-
Evaluation of Low-Value Services Across Major Medicare Advantage Insurers and Traditional Medicare.JAMA Netw Open. 2024 Nov 4;7(11):e2442633. doi: 10.1001/jamanetworkopen.2024.42633. JAMA Netw Open. 2024. PMID: 39485350 Free PMC article.
-
Use and Costs of Supplemental Benefits in Medicare Advantage, 2017-2021.JAMA Netw Open. 2025 Jan 2;8(1):e2454699. doi: 10.1001/jamanetworkopen.2024.54699. JAMA Netw Open. 2025. PMID: 39808428 Free PMC article.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
References
-
- Centers for Medicare & Medicaid Services. When can I buy a Medigap policy? Accessed December 19, 2024. https://www.medicare.gov/health-drug-plans/medigap/ready-to-buy/when
-
- Freed M, Biniek JF, Damico A, Neuman T. Medicare Advantage in 2024: enrollment update and key trends. KFF. August 8, 2024. Accessed September 4, 2024. https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2023-enro...
-
- Lipschutz D. Senate Finance Committee holds hearing on Medicare Advantage marketing misconduct. Center for Medicare Advocacy. October 19, 2023. Accessed December 19, 2024. https://medicareadvocacy.org/senate-finance-committee-holds-hearing-on-m...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
