

Computational fluid dynamics of small airway disease in chronic obstructive pulmonary disease
- PMID: 40174553
- PMCID: PMC11999283
- DOI: 10.1016/j.ebiom.2025.105670
Computational fluid dynamics of small airway disease in chronic obstructive pulmonary disease
Abstract
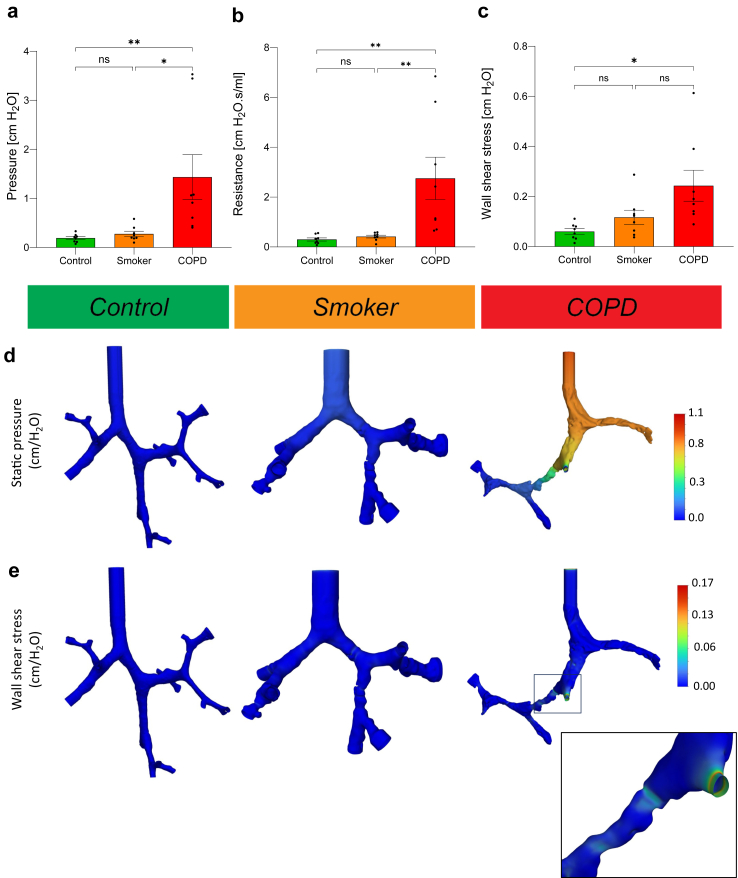
Background: Small airways (<2 mm diameter) are major sites of airflow obstruction in chronic obstructive pulmonary disease (COPD). This study aimed to quantify the impact of small airway disease, characterized by narrowing, occlusion, and obliteration, on airflow parameters in smokers and end-stage patients with COPDs.
Methods: We performed computational fluid dynamics (CFD) simulations of inspiratory airflow in three lung groups: control non-used donor lungs (no smoking/emphysema history), non-used donor lungs with a smoking history and emphysema, and explanted end-stage COPD lungs. Each group included four lungs, with two tissue cylinders. Micro-CT-scanned small airways were segmented into 3D models for CFD simulations to quantify pressure, resistance, and shear stress. CFD results were benchmarked against simplified linear and Weibel models.
Findings: CFD simulations showed higher pressures in COPD vs. controls (p = 0.0091) and smokers (p = 0.015), along with increased resistance (p = 0.0057 vs. controls; p = 0.0083 vs. smokers) and up to a tenfold rise in shear stress (p = 0.010 vs. controls). Narrowing and occlusion were shown to independently increase pressure, resistance, and shear stress, which were validated through segmentation corrections. Pressures and resistance assessed with simplified models were up to seven-fold higher for smokers and even 72 higher for COPD compared with CFD values.
Interpretation: These findings show that increased airflow parameters can explain the association between small airway disease and airflow limitation in COPD, underscoring small airway vulnerability. Additionally, they highlight the limitations of theoretical models in accurately capturing small airway disease.
Funding: Supported by the KU Leuven (C16/19/005).
Keywords: Airway remodelling; Airway resistance; Chronic obstructive pulmonary disease (COPD); Computational fluid dynamics (CFD); Obstruction; Small airway disease.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests BMV, WJ, WW, GGR are supported by the KU Leuven (C16/19/005). LJC received a grant and consulting fees from Medtronic, MSC received payment or honoraria to the institution from Vertex Pharmaceuticals and is an unpaid member of the advisory board on PCDResearch.org. VG, CH, IG, PK, MV, XJ and JV are junior research fellows and RV is a senior research fellow supported by the Research Foundation Flanders (11L9824N, 1152225N, 11N3922N, 1120425N, 1SE4322N, 11PGT24N,1803521N, 1160025N). MV received compensation from Sanofi for attending ERS2023 congress. SE received grants from Chiesi, consulting fees from GSK, payments or honoraria from GSK, Chiesi, Astra Zeneca and ALK and support for attending meetings from GSK, Sanofi and Astra Zeneca. JJ declares funding from the Wellcome Trust, Gilead, Microsoft Research, GSK, Cancer Research UK, Rosetrees Trust and Cystic Fibrosis trust; consulting fees from Boehringer Ingelheim, Roche, GSK, NHSX; payment for honoraria received from Boehringer Ingelheim, Roche, GlaxoSmithKline, Takeda; support for attending meetings and/or travel from Boehringer Ingelheim; patents planned, issued or pending (UK patent application number 2113765.8 and UK patent application number GB2211487.0); participation on a Data Safety Monitoring Board or Advisory Board for Boehringer Ingelheim and Roche.
Figures





References
-
- Hogg J.C., Chu F., Utokaparch S., et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:2645–2653. - PubMed
-
- Weibel E.R. Springer Berlin Heidelberg; Berlin, Heidelberg: 1963. Morphometry of the human lung. - DOI
-
- Pedley T.J., Schroter R.C., Sudlow M.F. The prediction of pressure drop and variation of resistance within the human bronchial airways. Respir Physiol. 1970;9:387–405. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
