

State of health and inequalities among Italian regions from 2000 to 2021: a systematic analysis based on the Global Burden of Disease Study 2021
- PMID: 40175012
- PMCID: PMC11962357
- DOI: 10.1016/S2468-2667(25)00045-3
State of health and inequalities among Italian regions from 2000 to 2021: a systematic analysis based on the Global Burden of Disease Study 2021
Abstract
Background: Over the past two decades, the Italian National Health Service has been gradually decentralised, with Italy's 21 regional governments now responsible for managing their health services. This change, coupled with austerity measures and a steadily ageing population, has adversely affected universal health coverage and equity, exacerbating inequalities and regional disparities. This study aimed to analyse time trends and subnational differences in the burden of disease from 2000 to 2019, and from 2019 to 2021 to capture the effects of the COVID-19 pandemic.
Methods: This study uses estimates for Italy from the Global Burden of Diseases, Injuries, and Risk Factors Study 2021. We analyse trends and geographical differences in disease burden from 2000 to 2021. Metrics include life expectancy, health-adjusted life expectancy (HALE), years lived with disability (YLDs), years of life lost (YLLs), and disability-adjusted life-years (DALYs) observed at national, macroregional, and subnational levels. Percent changes in rates, with both all-age and age-standardised rates, and 95% uncertainty intervals (95% UIs) are reported.
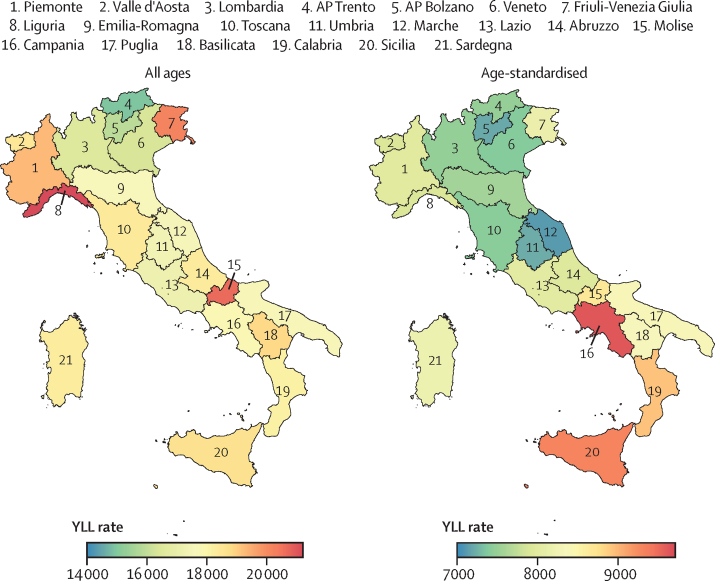
Findings: Life expectancy at birth in Italy increased from 79·6 years in 2000 to 83·4 years in 2019, dropped to 82·2 years in 2020 due to COVID-19, and recovered slightly to 82·7 years in 2021. HALE was 70·9 years (95% UI 67·4-73·8) in 2021. Substantial regional disparities were observed: in general, despite higher YLD rates, northern regions had better health outcomes, with higher life expectancy and HALE and lower YLL rates compared with southern regions. Overall, the top causes of YLDs were low back pain (1556·5 [1098·5-2080·2]), falls (926·2 [638·8-1253·8]), and headache disorders (858·0 [173·7-1808·2]). Anxiety and depressive disorders both had substantial increases in the period from 2019 to 2021 (19·8% and 17·3%, respectively). YLDs for Alzheimer's disease and diabetes increased substantially from 2000 to 2019 and 2019 to 2021 (70·6% and 3·0% for Alzheimer's disease and 46·8% and 7·9%, respectively for each timepoint). YLL rates declined for ischaemic heart disease from 2000 (-29·9% in 2019), but increased for Alzheimer's disease and other dementias (54·5%). DALY rates decreased overall from 2000 to 2019, but rose again in 2021 due to the COVID-19 pandemic.
Interpretation: The study highlights considerable regional disparities in Italy's health outcomes, driven by demography, heterogeneous health service quality, and economic inequalities. Addressing the increasing burden of Alzheimer's disease, diabetes, and mental health disorders, as well as regional disparities, requires strengthened preventive measures, equitable health service access, and socioeconomic policies, both at the national and regional levels.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2025 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests FB declares the position of Secretary of International Commission on Occupational Health Scientific Committee on Cardiology in Occupational Health. MBe declares payment or honoraria from Lundbeck and Angelini. ML declares payment for attending meetings or travel from the European Academy of Neurology Society of Neurology and from the Italian Society of Neurology. GZ, LGM, LMo, and LR declare payments to their institutions from the Italian Ministry of Health in support of this work. RaP declares grants or contracts from the UK Multiple Sclerosis Society and payment or honoraria from Biogen, MSD, Sanofi, and BMS. RoP declares membership of a data safety monitoring board for Fondazione Italiana Linfomi–ETS; an unpaid leadership role at the European Society for Blood and Marrow Transplantation; and past membership of the IRB/IEC Comiato Etico AO SS. SS declares grants or contracts with Novartis and Uriach; consulting fees and payments or honoraria from Novartis, Allergan (AbbVie), Teva, Lilly, Lundbeck, Pfizer, Novo Nordisk, Abbott, and AstraZeneca; support for attending a meeting or travel costs from Lilly, Novartis, Teva, Lundbeck, and Pfizer; receipt of medical equipment, drugs, or materials from Allergan (AbbVie) and Novo Nordisk; and is President of the European Stroke Organisation and Editor-in-Chief of Cephalalgia. DT declares payments or honoraria from AstraZeneca, Eli Lilly, and Novo Nordisk; support for attending meetings or travel from AstraZeneca, participation on data safety monitoring boards at Amarin, Npejringer Ingelheim, and Novo Nordisk; receipt of medical equipment, drugs, or materials from Abbott and PharmaNutra; and leadership roles at the European Association for the Study of Diabetes Early Career Academy and Committee on Clinical Affairs.
Figures




References
-
- Ferre F, de Belvis AG, Valerio L, et al. Italy: health system review. Health Syst Transit. 2014;16:1–168. - PubMed
-
- Chernew ME, Baicker K, Hsu J. The specter of financial armageddon–health care and federal debt in the United States. N Engl J Med. 2010;362:1166–1168. - PubMed
-
- Hagist C, Kotlikoff LJ. Who's going broke? Comparing growth in public healthcare expenditure in ten OECD countries. Hacienda Publica Espanola/Revista de Economia Publica. 2009;188:55–72.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
