

Effect of surface inclination and gluteus maximus activation on lumbar lordosis and footpronation in individuals with low back pain with extension pattern: a preliminary study
- PMID: 40175504
- PMCID: PMC11965470
- DOI: 10.1038/s41598-025-96048-w
Effect of surface inclination and gluteus maximus activation on lumbar lordosis and footpronation in individuals with low back pain with extension pattern: a preliminary study
Abstract
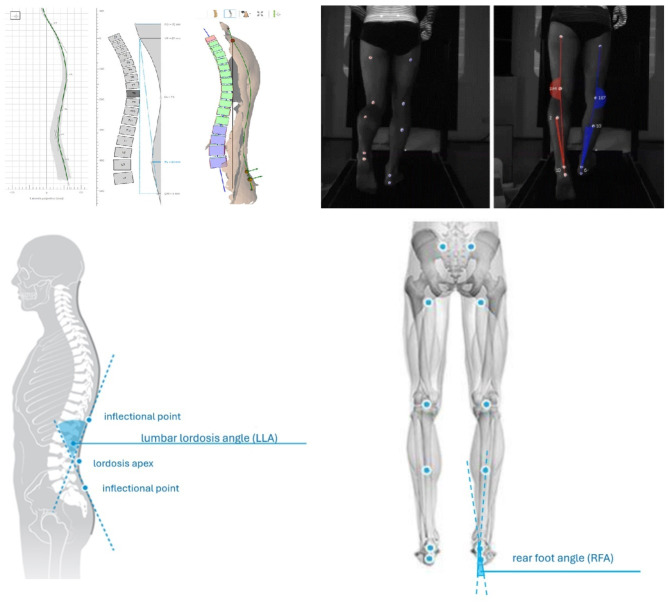
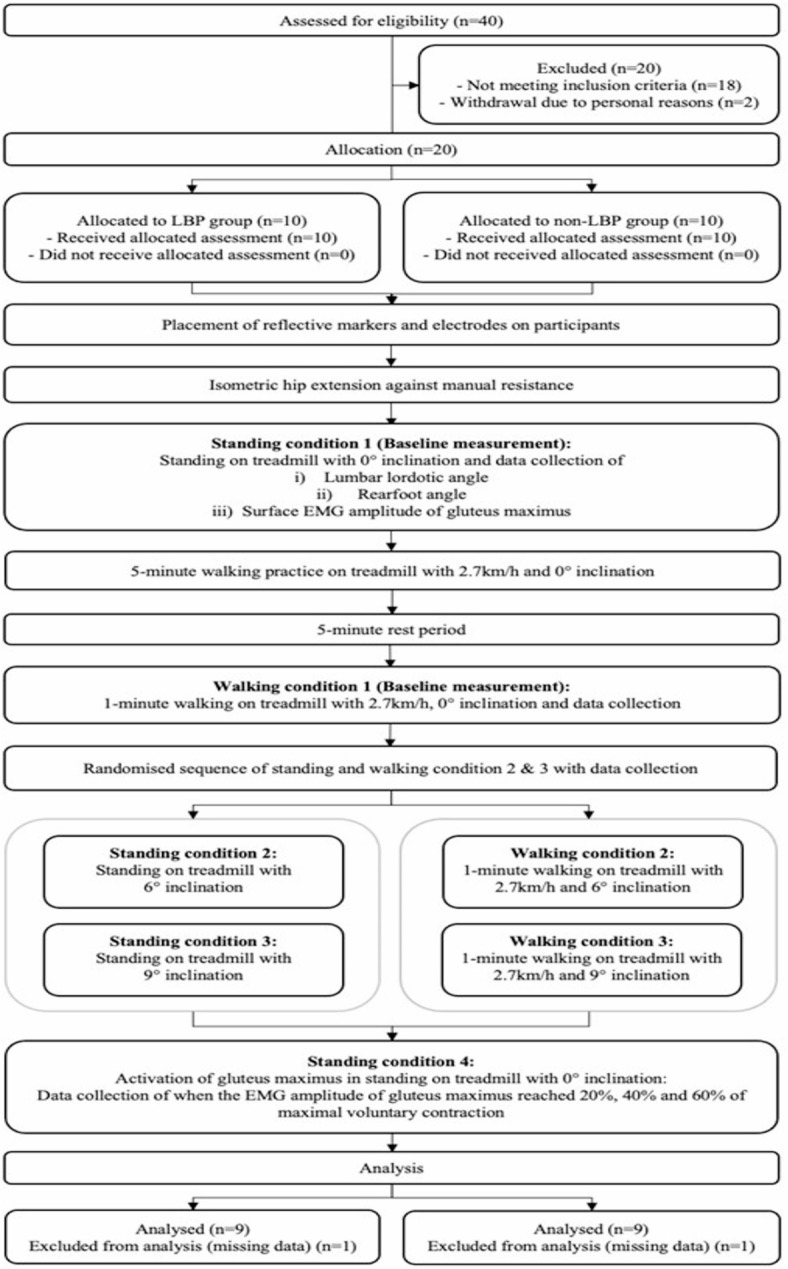
Lumbar hyperlordosis and foot overpronation are associated with low back pain with extension pattern. This study examined if standing and walking on inclined surface or gluteus maximus activation alleviates the extent of lumbar lordosis and foot pronation amongst individuals with LBP who were classified with extension pattern. Eighteen adults with foot overpronation (LBP group, n = 9 and non-LBP group, n = 9) participated in this cross-sectional and case-control comparison study. Lumbar lordotic angle and rearfoot angle were measured using surface tomography, during standing and walking on treadmill at inclinations of 0°, 6° and 9°, and voluntary gluteus maximus activation at 20%, 40% and 60% of maximal contraction in standing at 0° inclination. The lumbar lordosis angle and rearfoot angle were compared within-group and between two groups across the listed trials in standing and walking. Results indicated no significant change in lumbar lordosis or rearfoot angle in LBP group when standing or walking on 6°or 9°inclined surface (p > 0.05). However, voluntary gluteus maximus activation in standing at the level of 20%, 40% and 60% of maximal effort reduced lumbar lordotic angle (p < 0.05) but not rearfoot angle (p > 0.05) in LBP group. Our findings provide a novel approach to address the hyperlordosis in LBP group with extension pattern, for which voluntary gluteus maximus activation of ≥ 20% of maximal effort could effectively reduce the extent of the lumbar lordosis in level-ground standing in the LBP group. Such modified lumbar posture may alleviate the compressive loading on the spine associated with static upright standing at our daily activities. Increased gluteus maximus activation found during inclined walking may be beneficial to those with LBP and extension pattern.
Keywords: Foot pronation; Gluteus Maximus; Inclined surface; Lordosis; Low back pain.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
The impact of different standing positions on gluteus medius activation and lumbar lordosis in LBP-developers during prolonged standing.PLoS One. 2025 Feb 11;20(2):e0317291. doi: 10.1371/journal.pone.0317291. eCollection 2025. PLoS One. 2025. PMID: 39932988 Free PMC article.
-
The relationship between lumbar lordosis angle and low back pain in individuals with transfemoral amputation.Prosthet Orthot Int. 2019 Apr;43(2):227-232. doi: 10.1177/0309364618792746. Epub 2018 Aug 18. Prosthet Orthot Int. 2019. PMID: 30122108
-
Effect of Lumbar Disc Degeneration and Low-Back Pain on the Lumbar Lordosis in Supine and Standing: A Cross-Sectional MRI Study.Spine (Phila Pa 1976). 2015 Nov;40(21):1690-6. doi: 10.1097/BRS.0000000000001120. Spine (Phila Pa 1976). 2015. PMID: 26502098
-
Immediate effects of a rucksack type orthosis on the elderly with decreased lumbar lordosis during standing and walking.Electromyogr Clin Neurophysiol. 2008 Jan-Feb;48(1):53-61. Electromyogr Clin Neurophysiol. 2008. PMID: 18338535 Clinical Trial.
-
Postural asymmetry in low back pain - a systematic review and meta-analysis of observational studies.Disabil Rehabil. 2025 Apr;47(7):1659-1676. doi: 10.1080/09638288.2024.2385070. Epub 2024 Aug 21. Disabil Rehabil. 2025. PMID: 39166267
References
-
- Sheeran, L., Sparkes, V., Whatling, G., Biggs, P. & Holt, C. Identifying non-specific low back pain clinical subgroups from sitting and standing repositioning posture tasks using a novel Cardiff Dempster–Shafer theory classifier. Clin. Biomech. Elsevier Ltd. 70, 237–244. 10.1016/j.clinbiomech.2019.10.004 (2019). - PMC - PubMed
-
- Vogt, L., Pfeifer, K. & Banzer, W. Neuromuscular control of walking with chronic low-back pain. Man. Ther.810.1054/math.2002.0476 (2003). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
