

Altered metabolic profiles in colon and rectal cancer
- PMID: 40175601
- PMCID: PMC11965280
- DOI: 10.1038/s41598-025-96004-8
Altered metabolic profiles in colon and rectal cancer
Abstract
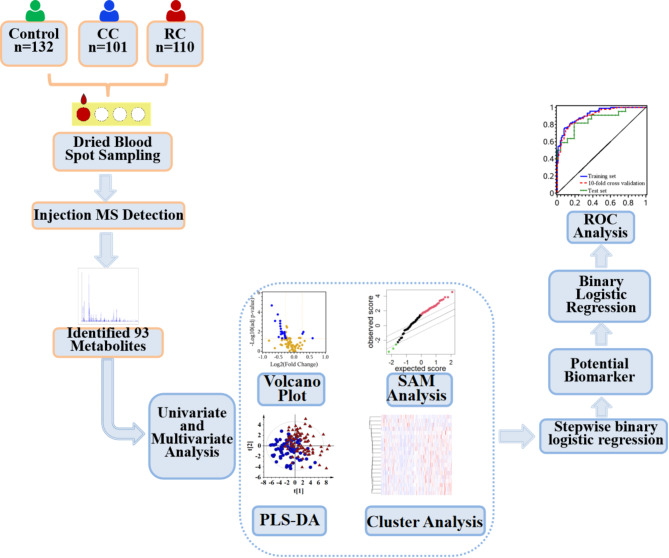
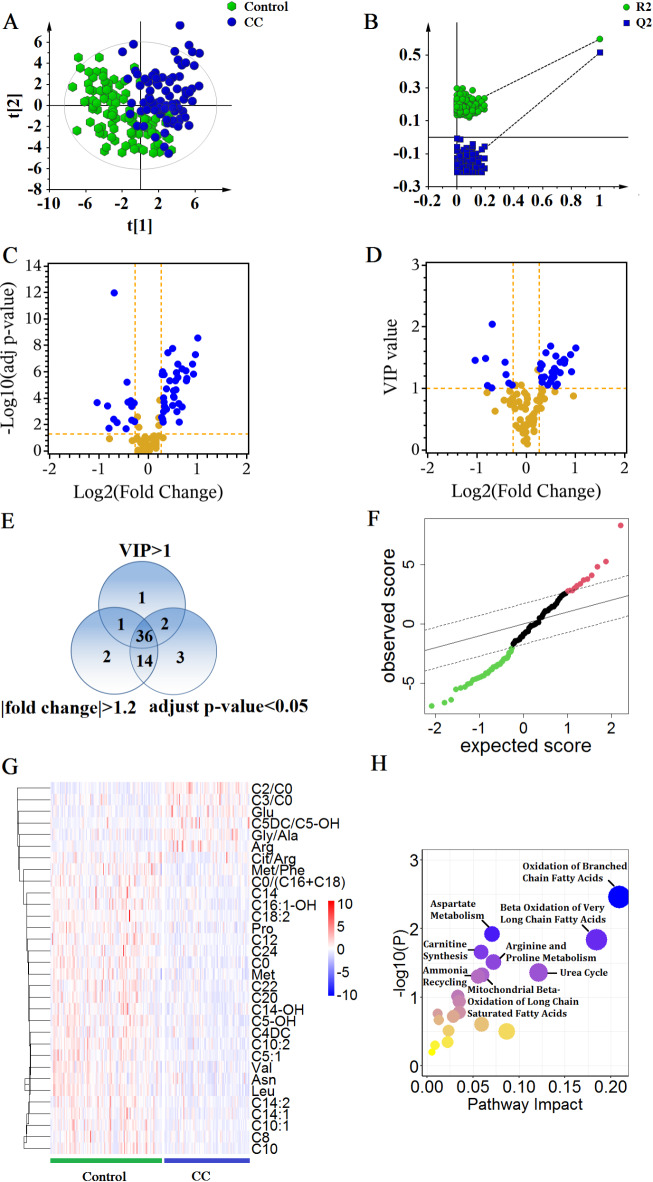
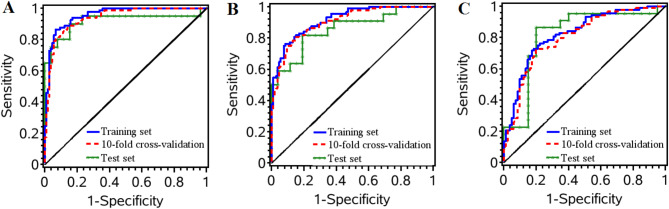
Colorectal cancer (CRC) is the third most commonly diagnosed malignant tumour in worldwide populations. Although colon cancer (CC) and rectal cancer (RC) are often discussed together, there is a global trend towards considering them as two separate disease entities. It is necessary to choice the appropriate treatment for CC and RC based on their own characteristics. Hence, it is a great importance to find effective biomarkers to distinguish CC from RC. In the present study, a total of 343 participants were recruited, including 132 healthy individuals, 101 patients with CC, and 110 patients with RC. The concentrations of 93 metabolites were determined by using a combination of dried blood spot sampling and direct infusion mass spectrometry technology. Multiple algorithms were applied to characterize altered metabolic profiles in CC and RC. Significantly altered metabolites were screened for distinguishing RC from CC in training set. A biomarker panel including Glu, C0, C8, C20, Gly/Ala, and C10:1 was tested with tenfold cross-validation and an independent test set, and showed the potential to distinguish between RC and CC. The metabolomics analysis makes contribution to summarize the metabolic differences in RC and CC, which might provide further guidance on novel clinical designs for the two diseases.
Keywords: Colon cancer; Dried blood spot sampling; Mass spectrometry; Metabolomics; Rectal cancer.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Institutional review board statement: This study was approved by Ethics Committee of the First Affiliated Hospital of Jinzhou Medical University. Informed consent: This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was provided from each research participants.
Figures


References
-
- Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71 (3), 209–249 (2021). - PubMed
-
- Bray, F. et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.68 (6), 394–424 (2018). - PubMed
-
- Fathi, M. et al. T-cell Immunoglobulin and ITIM domain, as a potential immune checkpoint target for immunotherapy of colorectal cancer. IUBMB Life. 73 (5), 726–738 (2021). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
