

Unravelling a pediatric enigma: coexisting retroesophageal right subclavian artery and congenital colonic stenosis masquerading as cow's milk protein allergy and ileus in a neonate
- PMID: 40175956
- PMCID: PMC11967120
- DOI: 10.1186/s12887-025-05642-4
Unravelling a pediatric enigma: coexisting retroesophageal right subclavian artery and congenital colonic stenosis masquerading as cow's milk protein allergy and ileus in a neonate
Abstract
Background: Double alimentary tract obstruction due to congenital anomalies is a rare clinical occurrence, with limited cases published in medical literature. This article presents a unique case of coexisting retroesophageal right subclavian artery (RRSA) and congenital colonic stenosis (CCS), conditions that have not been previously documented together in pediatric population.
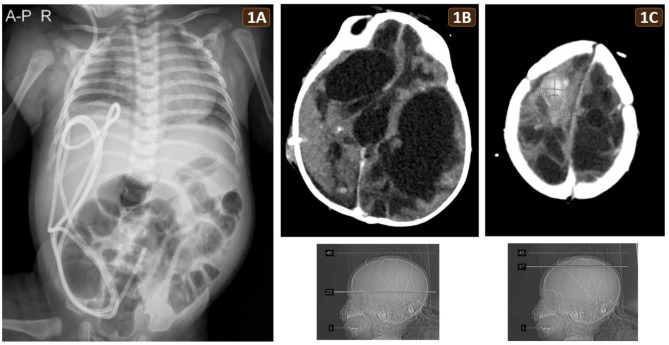
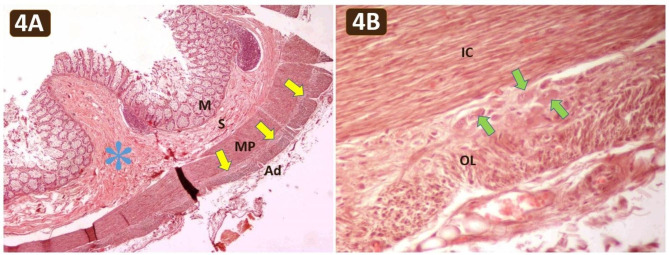
Case presentation: A Thai male newborn was born by cesarean section at gestational age of 41 weeks. One week before birth, intrauterine asphyxia and idiopathic bilateral intracerebral hemorrhage were diagnosed by prenatal ultrasonography. Despite postnatal interventions including a ventriculoperitoneal shunt and subsequent external ventricular drain, the intracerebral hemorrhage recurred and progressed. Concurrently, the patient experienced multiple episodes of post-feeding vomiting, intermittent abdominal distension, and regular defecation without constipation. Sepsis secondary to an infected shunt occurred, accompanied by marked abdominal distension. The physician clinically suspected non-IgE-mediated cow's milk protein allergy and ileus associated with sepsis. Tragically, the patient succumbed at seven months due to a brain abscess stemming from an infected external ventricular drain. Ultimately, postmortem examination unraveled double alimentary tract obstruction, consisting of RRSA and CCS. The RRSA, originating from proximal thoracic aorta, caused notable esophageal compression and functional stenosis which led to the frequent vomiting and reflux. The CCS involved the distal transverse colon, descending colon and proximal sigmoid colon, accounting for nearly 50% of the colon. The CCS was therefore the exact cause of intermittent abdominal distension. The stenotic colon contained submucosal and myenteric plexuses, excluding Hirschsprung disease.
Conclusion: This case highlights the diagnostic complexities of RRSA and CCS resulting in double gut obstruction and masquerading as non-IgE-mediated cow's milk protein allergy and sepsis-induced ileus. Awareness of these rare coexisting congenital anomalies can aid in early recognition, prevent misdiagnosis, enable timely management and improve outcomes for affected pediatric patients.
Keywords: Abdominal distension; Congenital colonic stenosis; Cow's milk protein allergy; Gut obstruction; Ileus; Misdiagnosis; Neonatal vomiting; Reflux; Retroesophageal right subclavian artery; Sepsis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Formal informed consent for cadaver preservation, postmortem examination and publication of this case report was obtained [Cadaver donation number: 60030172 and R013/2560]. Approval for this project was granted by the head of the Department of Anatomy, Faculty of Science, Mahidol University. Consent for publication: Written informed consent for publication was obtained from the parents of the patient/cadaver. Competing interests: The authors declare no competing interests.
Figures


References
-
- Bayford D. An account of a singular case of obstructed deglutition. Mem Med Soc Lond. 1794;2:275–86.
-
- Schweighofer N, Dolinšek J, Rupreht M. Arteria lusoria as a cause of dysphagia in an infant. J Pediatr Health Care. 2023;37(6):702–5. 10.1016/j.pedhc.2023.07.001. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
