

Improved prediction and risk stratification of major adverse cardiovascular events using an explainable machine learning approach combining plasma biomarkers and traditional risk factors
- PMID: 40176039
- PMCID: PMC11966882
- DOI: 10.1186/s12933-025-02711-x
Improved prediction and risk stratification of major adverse cardiovascular events using an explainable machine learning approach combining plasma biomarkers and traditional risk factors
Abstract
Background: Cardiovascular diseases (CVD) remain the leading cause of morbidity and mortality globally. Traditional risk models, primarily based on established risk factors, often lack the precision needed to accurately predict new-onset major adverse cardiovascular events (MACE). This study aimed to improve prediction and risk stratification by integrating traditional risk factors with biochemical and metabolomic biomarkers.
Methods: We analyzed data from 229,352 participants in the UK Biobank (median age 58.0 years; 45.4% male) who were free of baseline MACE. Biomarker selection was conducted using area under the curve (AUC), minimal joint mutual information maximization (JMIM), and correlation analyses, while Cox proportional hazards models were employed to evaluate the predictive performance of combined traditional risk factors and biomarkers. Optimal binary thresholds were determined utilizing CatBoost and SHAP, leading to the calculation of a Biomarker Risk Score (BRS) for each participant. Multivariable Cox models were conducted to assess the associations of each concerned biomarker and BRS with new-onset endpoints.
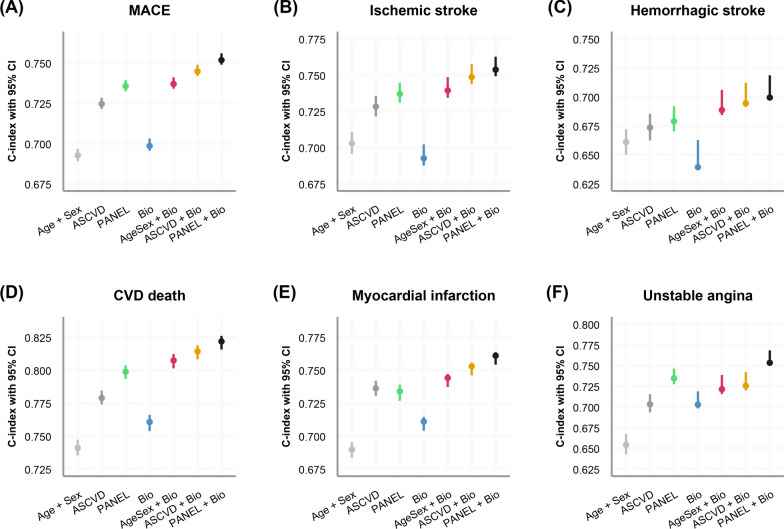
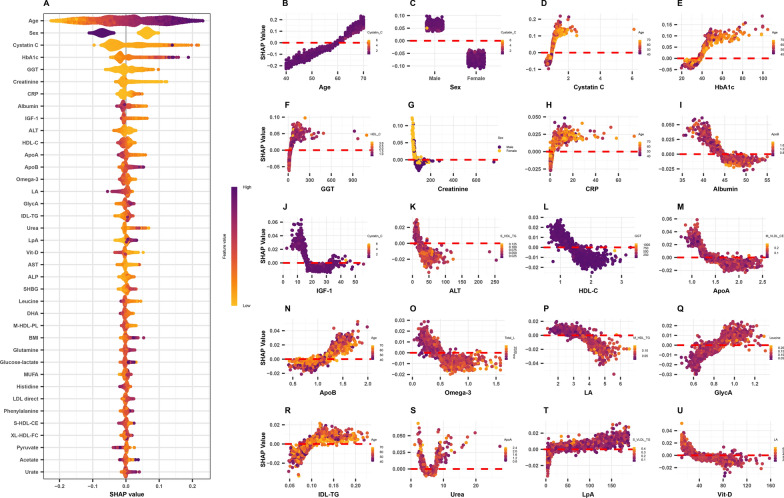
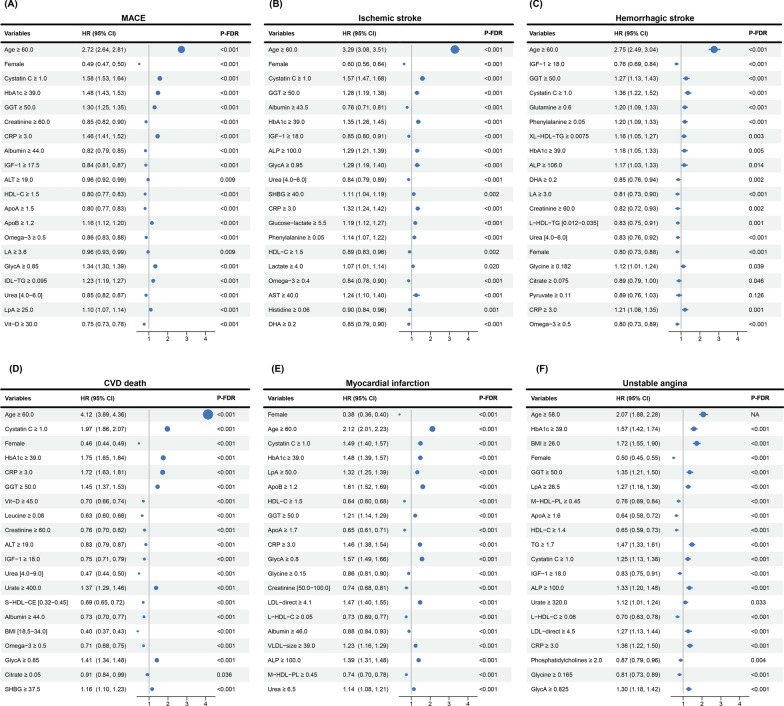
Results: The combination of PANEL + All Biochemistry + Cor0.95 of Nonov Met predictors demonstrated significantly improved discriminative performance compared to traditional models, such as Age + Sex and ASCVD, across all endpoints. Although the prediction for hemorrhagic stroke was suboptimal (C-index = 0.699), C-index values for other outcomes surpassed 0.75, with the highest value (0.822) recorded for CVD-related mortality. Key predictors of new-onset MACE included cystatin C, HbA1c, GlycA, and GGT, while IGF-1 and DHA exhibited potential protective effects. The BRS stratified individuals into low-, intermediate-, and high-risk groups, with the strongest effect observed for CVD death, where the high-risk group had a relative risk of 2.76 (95% CI 2.48-3.07) compared to the low-risk group.
Conclusion: Integrating traditional risk factors and biomarkers improves prediction and risk stratification of new-onset MACE. The BRS shows promise as a tool for identifying high-risk individuals, with the potential to support personalized CVD prevention and management strategies.
Keywords: Binary threshold; Biomarker risk score; Cardiovascular research; Major adverse cardiovascular events; Risk stratification.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This research complied with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their involvement, and ethical approval was granted by the North West Multi-Center Research Ethics Committee (reference: 11/NW/0382; https://www.ukbiobank.ac.uk/learn-more-about-ukbiobank/about-us/ethics ). Any additional ethical approval was adjudged unnecessary for the present study. Patient and public involvement: Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research. Patient consent for publication: Not required. Competing interests: The authors declare no competing interests.
Figures



References
-
- Timmis A, Aboyans V, Vardas P, Townsend N, Torbica A, Kavousi M, et al. European Society of Cardiology: the 2023 Atlas of Cardiovascular Disease Statistics. Eur Heart J. 2024;45:4019–62. - PubMed
-
- Joynt Maddox KE, Elkind MSV, Aparicio HJ, Commodore-Mensah Y, de Ferranti SD, Dowd WN, et al. Forecasting the burden of cardiovascular disease and stroke in the United States through 2050-prevalence of risk factors and disease: a presidential advisory from the American Heart Association. Circulation. 2024;150:e65-88. - PubMed
-
- Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2935–59. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
