

Inequalities in paediatric hospitalisations for costly and prevalent conditions in Ontario, Canada: a population-based cohort study
- PMID: 40177389
- PMCID: PMC11964682
- DOI: 10.1016/j.lana.2025.101056
Inequalities in paediatric hospitalisations for costly and prevalent conditions in Ontario, Canada: a population-based cohort study
Abstract
Background: Identifying inequalities is important for informing research, and policy efforts to reduce health disparities. This study measured the inequalities in hospitalisations for the costly and prevalent conditions in hospitalised children using association estimates.
Methods: Population-based cohort study using health administrative databases in Ontario, Canada between 2014 and 2019. The hospitalisation rate was determined for the costly and prevalent conditions in children. Hospitalisation inequalities by four equity stratifiers (material resources, rurality, sex, and immigrant status) were quantified using rate difference (RD), rate ratio (RR), and ratio of excess to total hospitalisation rate. Multivariable logistic regression analyses were also conducted.
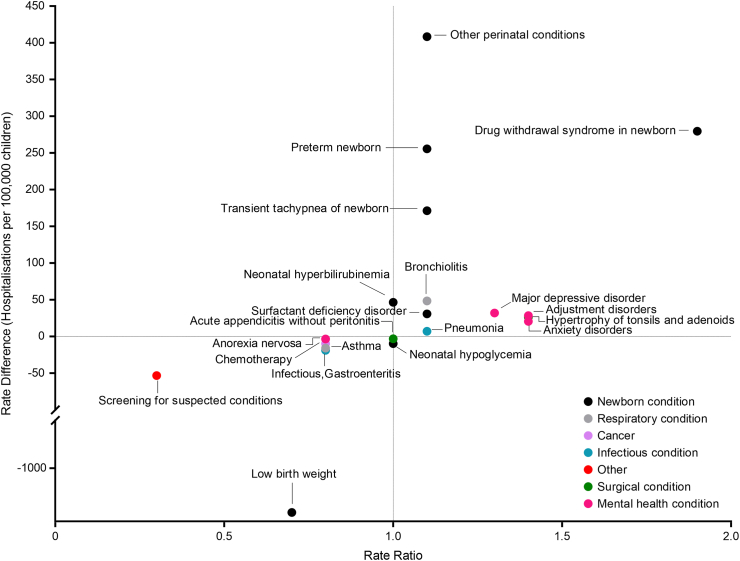
Findings: In a population of 3·7 million children (median age 7·0 years, Interquartile range: 1·0-12·0), there were 612,597 hospitalisations. Large inequalities comparing children among least versus most resourced quintile was observed in low birth weight (RD: 1,823·3 hospitalisations per 100,000 children, 95% CI: 1,662·7, 1,983·9). Conditions with large inequalities comparing rural versus urban areas included low birth weight (RD: -1,833·2 hospitalisations per 100,000, 95% CI: -2,012·8, -1,653·6); and drug withdrawal syndrome in newborn (RR: 1·9, 95% CI: 1·7, 2·1; adjusted odds ratio (aOR): 1·4, 95% CI: 1·2, 1·5). Conditions with large inequalities comparing males versus females included low birth weight (RD: -888·3 hospitalisations per 100,000, 95% CI: -992·5, -784·02); and anorexia nervosa (RR: 0·08, 95% CI: 0·07, 0·10; aOR: 0·1, 95% CI: 0.1, 0.1). Conditions with large inequalities comparing non-refugee immigrants versus non-immigrants included major depressive disorder (RR: 2·8, 95% CI: 2·7, 2·9), and comparing refugees versus non-immigrants included drug withdrawal syndrome in newborn (RR: 0·09, 95% CI: 0·05, 0·15). Results from multivariable analyses were similar.
Interpretation: Newborn and mental health conditions had the largest inequalities in hospitalisations by the equity stratifiers. Findings from this study can be used to prioritise future health equity research to reduce health inequalities.
Funding: PSI Foundation.
Keywords: Health inequalities; Hospitalisation; Immigrant status; Paediatric; Rurality; Sex; Socioeconomic status.
© 2025 The Author(s).
Conflict of interest statement
Dr. Gill has received grants from the Canadian Institute of Health Research (CIHR), the PSI Foundation, and The Hospital for Sick Children. Dr. Cohen is a member of the Committee to Evaluate Drugs which provides advice to Ontario's Ministry of Health on Public Drug Policy. All other authors declare no conflict of interest.
Figures




References
-
- World Health Organization . World Health Organization; Geneva: 2013. Handbook on Health Inequality Monitoring: With a Special Focus on Low- and Middle-income Countries.
-
- National Center for Health Statistics (US) National Center for Health Statistics; Hyattsville (MD): 2016. Health, United States, 2015: with special feature on racial and ethnic health disparities.https://www.ncbi.nlm.nih.gov/books/NBK367640/
-
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Community-Based Solutions to Promote Health Equity in the United States . National Academies Press (US); Washington, DC: 2017. Communities in Action: Pathways to Health Equity. - DOI
-
- World Health Organization . World Health Organization; Geneva: 2017. National Health Inequality Monitoring: A Step-by-step Manual. Licence: CC BY-NC-SA 3.0 IGO.
LinkOut - more resources
Full Text Sources
Miscellaneous
