

Insulin-like growth factor binding protein-3 (IGFBP-3): a biomarker of coronary artery disease induced myocardial ischaemia
- PMID: 40177504
- PMCID: PMC11961406
- DOI: 10.1093/ehjopen/oeaf028
Insulin-like growth factor binding protein-3 (IGFBP-3): a biomarker of coronary artery disease induced myocardial ischaemia
Abstract
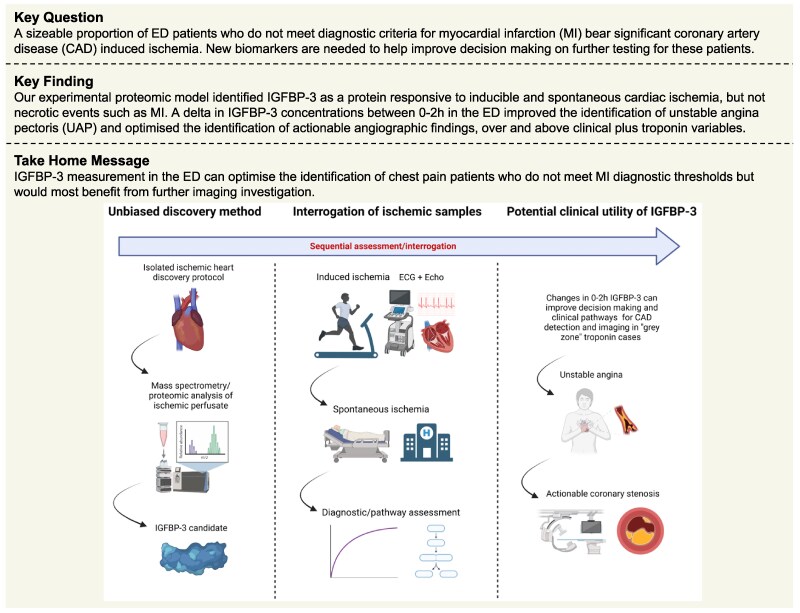
Aims: Among individuals presenting to the emergency department (ED) with chest pain, clinical uncertainty surrounds the appropriate identification of non-myocardial infarction (MI) individuals who would most benefit from objective functional/anatomical testing (e.g. imaging). We applied a proteomic biomarker discovery approach to identify novel candidates reflecting coronary artery disease (CAD) induced ischaemia that could translate to measurement in clinical samples.
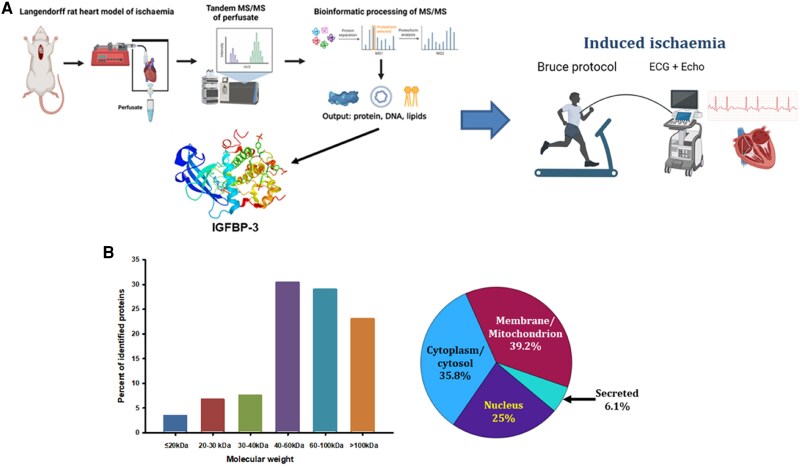
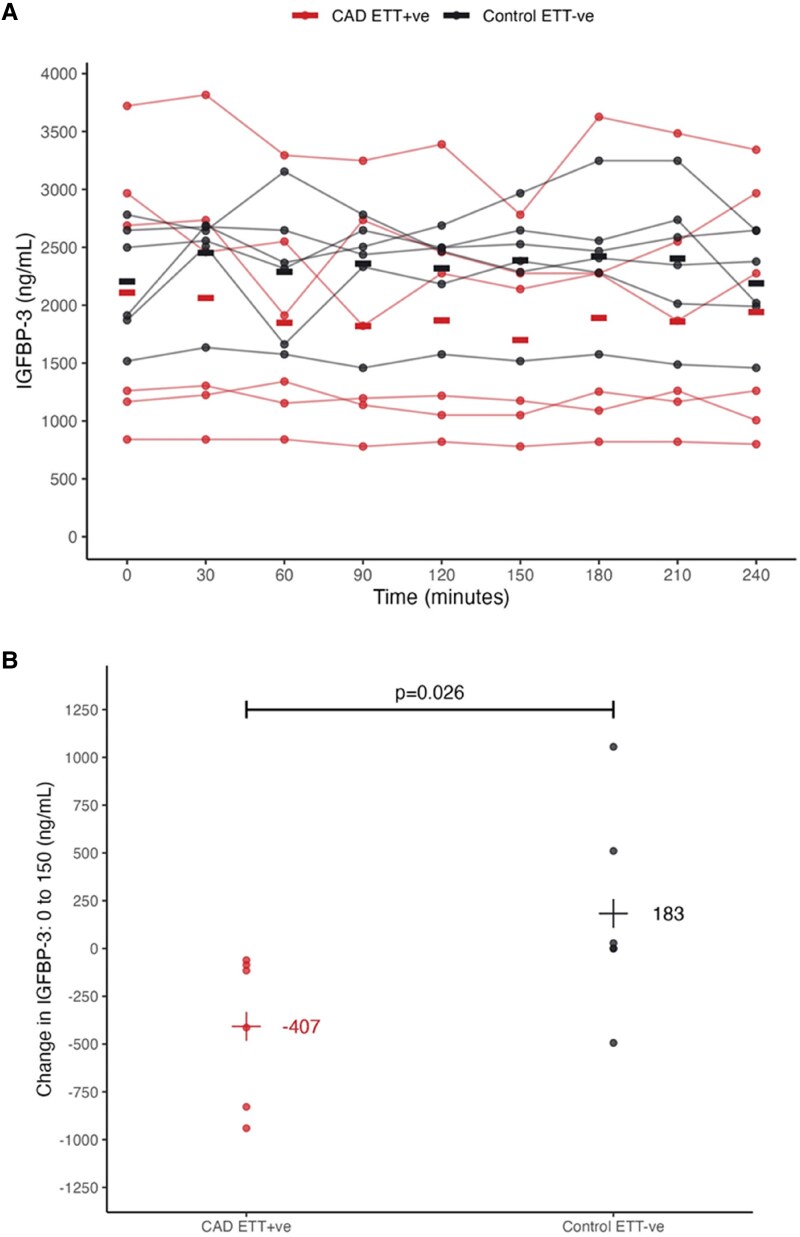
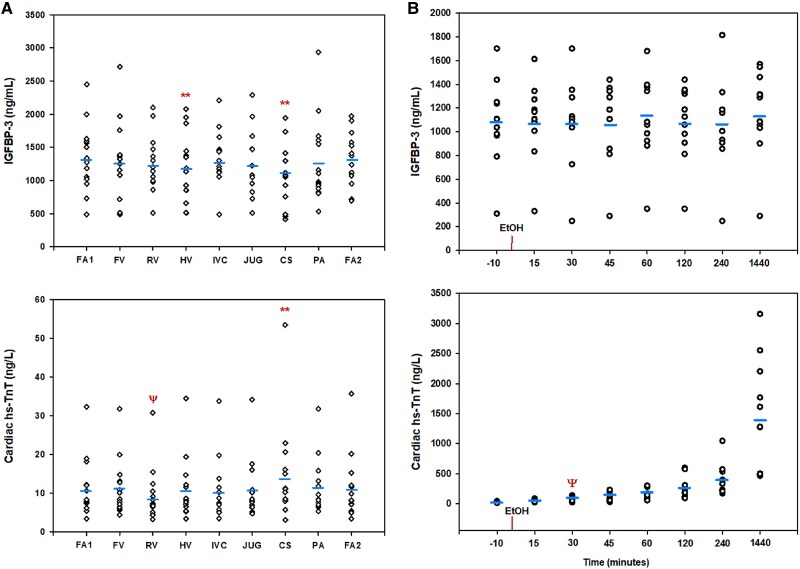
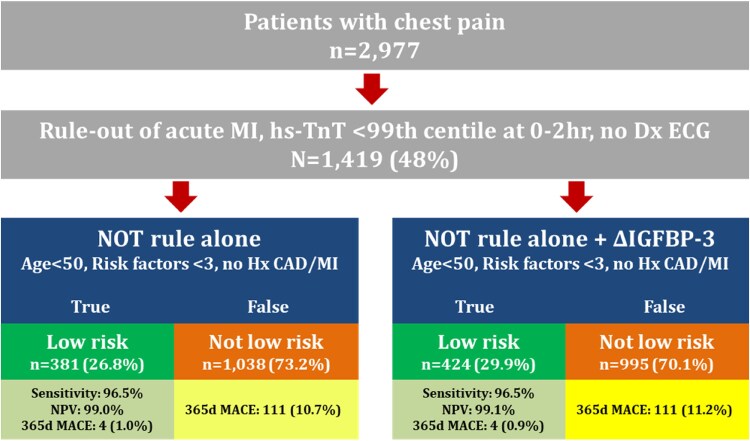
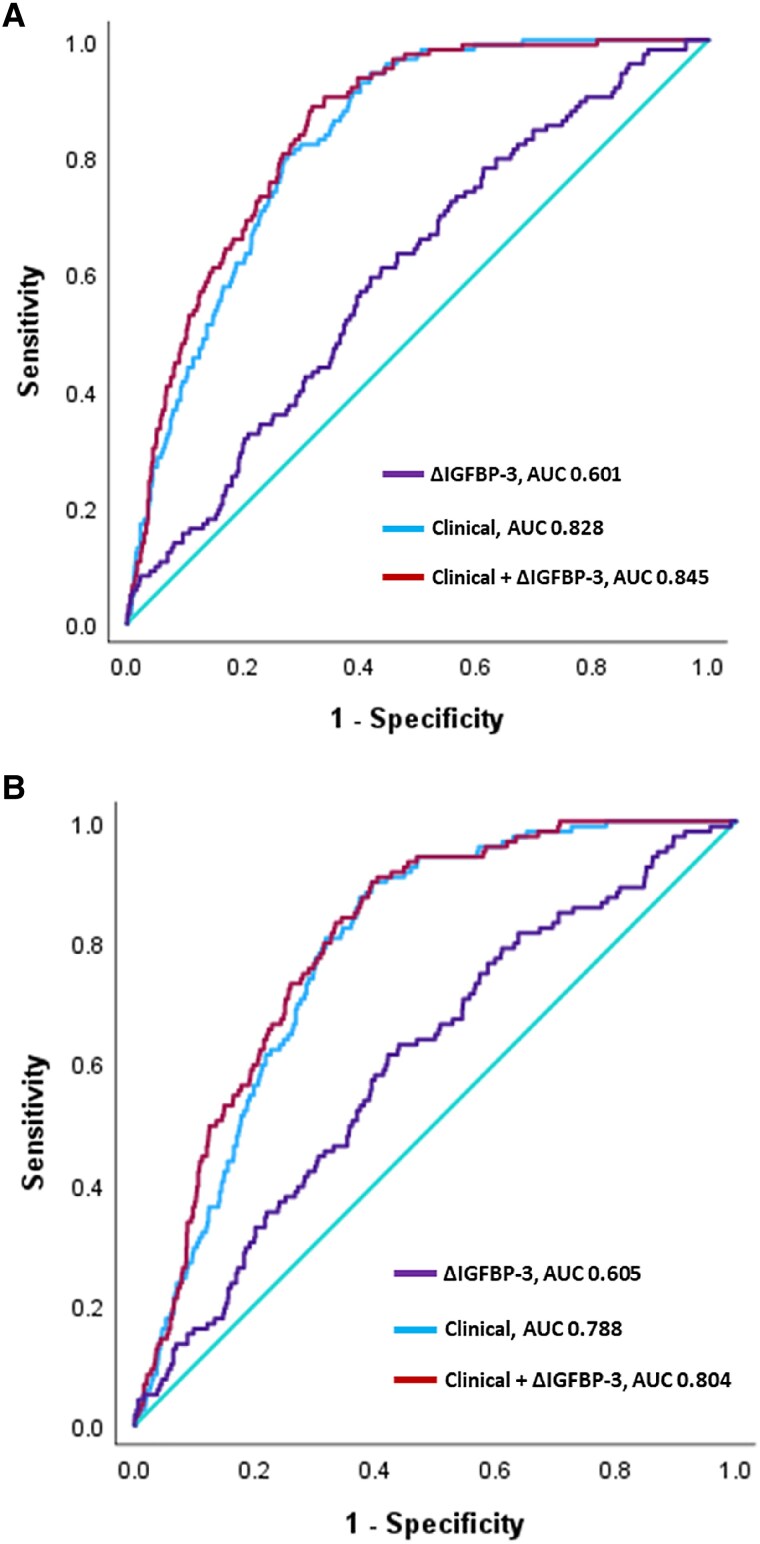
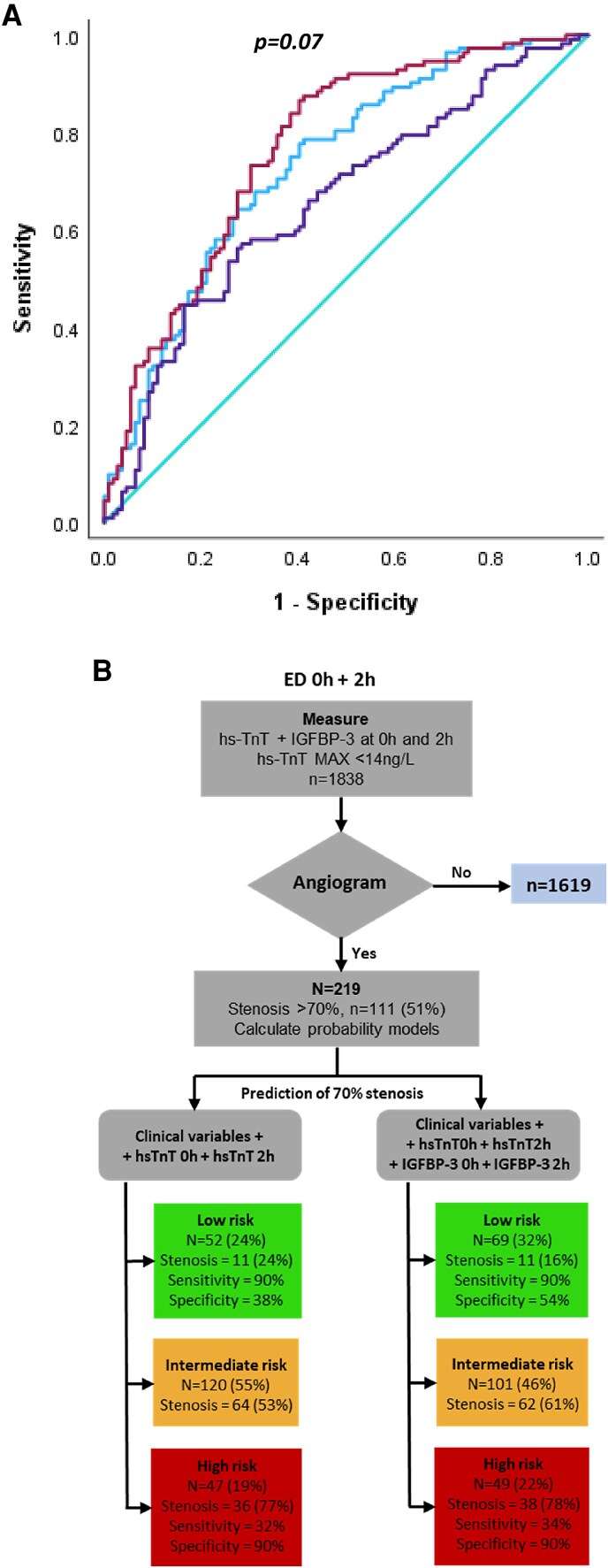
Methods and results: Mass spectroscopy (MS) of perfusate from an isolated rat heart model of cardiac ischaemia identified >100 novel protein biomarkers. A prominent candidate, insulin-like growth factor binding protein (IGFBP-3), was then interrogated for its ability to identify CAD-related ischaemia (e.g. positive cardiac stress test; unstable angina pectoris, UAP; arterial stenosis >70% on angiography) in multiple patient sample sets [cardiac stress testing, n = 12; septal alcohol ablation (SAA), n = 12; ED chest pain, n = 2977]. In cardiac stress testing, a significant delta IGFBP-3 (ΔIGFBP-3) between 0 and 150 min was seen in positive, but not negative, tests (P = 0.03). In SAA, peripheral IGFBP-3 levels did not change over 24 h (P = 0.57). In ED patients, ΔIGFBP-3 between 0 and 2 h (i) identified more 365-day low-risk major adverse cardiac event cases (27-30%), (ii) provided 7% improvement in positive predictive value over a clinical model for the identification of unstable angina (P = 0.01), and (iii) was a significant, independent predictor of >70% stenosis on angiography, improving indeterminate risk prediction by 9% (95% CI 3-15%).
Conclusion: Our discovery approach has translated IGFBP-3 as a potential biomarker to identify significant CAD/ischaemia in patients who do not meet diagnostic thresholds for MI.
Keywords: Acute coronary syndromes; Biomarker; CAD; IGFBP-3; Imaging; Troponin.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: J.W., J.P., K.J., and C.J.P. are employed by Upstream Medical Technologies. J.W., J.P., K.J., and C.J.P. have shares/options in UMT, as well as direct employ. C.J.P. and K.J. are listed as inventors of IP related to this report.
Figures
Similar articles
-
High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: results from the ROMICAT-II trial.J Am Coll Cardiol. 2014 Aug 19;64(7):684-92. doi: 10.1016/j.jacc.2014.05.039. J Am Coll Cardiol. 2014. PMID: 25125300 Free PMC article. Clinical Trial.
-
Insulin-like growth factor-binding protein 7 (IGFBP 7) as a new biomarker in coronary heart disease.Adv Med Sci. 2019 Mar;64(1):195-201. doi: 10.1016/j.advms.2018.08.017. Epub 2019 Feb 13. Adv Med Sci. 2019. PMID: 30769262
-
Increased deformation of the left ventricle during exercise test measured by global longitudinal strain can rule out significant coronary artery disease in patients with suspected unstable angina pectoris.Echocardiography. 2022 Feb;39(2):233-239. doi: 10.1111/echo.15295. Epub 2022 Jan 18. Echocardiography. 2022. PMID: 35043455
-
ESR Essentials: imaging in stable chest pain - practice recommendations by ESCR.Eur Radiol. 2024 Oct;34(10):6559-6567. doi: 10.1007/s00330-024-10739-y. Epub 2024 Apr 16. Eur Radiol. 2024. PMID: 38625611 Review.
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
References
-
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, Claeys MJ, Dan GA, Dweck MR, Galbraith M, Gilard M, Hinterbuchner L, Jankowska EA, Jüni P, Kimura T, Kunadian V, Leosdottir M, Lorusso R, Pedretti RFE, Rigopoulos AG, Rubini Gimenez M, Thiele H, Vranckx P, Wassmann S, Wenger NK, Ibanez B; ESC Scientific Document Group . 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44:3720–3826. - PubMed
-
- Twerenbold R, Costabel JP, Nestelberger T, Campos R, Wussler D, Arbucci R, Cortes M, Boeddinghaus J, Baumgartner B, Nickel CH, Bingisser R, Badertscher P, Puelacher C, du Fay de Lavallaz J, Wildi K, Rubini Giménez M, Walter J, Meier M, Hafner B, Lopez Ayala P, Lohrmann J, Troester V, Koechlin L, Zimmermann T, Gualandro DM, Reichlin T, Lambardi F, Resi S, Alves de Lima A, Trivi M, Mueller C. Outcome of applying the ESC 0/1-hour algorithm in patients with suspected myocardial infarction. J Am Coll Cardiol 2019;74:483–494. - PubMed
-
- Chiang CH, Chiang CH, Pickering JW, Stoyanov KM, Chew DP, Neumann JT, Ojeda F, Sörensen NA, Su KY, Kavsak P, Worster A, Inoue K, Johannessen TR, Atar D, Amann M, Hochholzer W, Mokhtari A, Ekelund U, Twerenbold R, Mueller C, Bahrmann P, Buttinger N, Dooley M, Ruangsomboon O, Nowak RM, DeFilippi CR, Peacock WF, Neilan TG, Liu MA, Hsu WT, Lee GH, Tang PU, Ma KS, Westermann D, Blankenberg S, Giannitsis E, Than MP, Lee CC. Performance of the European Society of Cardiology 0/1-hour, 0/2-hour, and 0/3-hour algorithms for rapid triage of acute myocardial infarction: an international collaborative meta-analysis. Ann Intern Med 2022;175:101–113. - PubMed
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, Blankstein R, Boyd J, Bullock-Palmer RP, Conejo T, Diercks DB, Gentile F, Greenwood JP, Hess EP, Hollenberg SM, Jaber WA, Jneid H, Joglar JA, Morrow DA, O'Connor RE, Ross MA, Shaw LJ. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;144:e368–e454. - PubMed
-
- Greenslade JH, Parsonage W, Than M, Scott A, Aldous S, Pickering JW, Hammett CJ, Cullen L. A clinical decision rule to identify emergency department patients at low risk for acute coronary syndrome who do not need objective coronary artery disease testing: the no objective testing rule. Ann Emerg Med 2016;67:478–489.e2. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
