

Critical Illness, Major Surgery, and Other Hospitalizations and Active and Disabled Life Expectancy
- PMID: 40178853
- PMCID: PMC11969285
- DOI: 10.1001/jamanetworkopen.2025.4208
Critical Illness, Major Surgery, and Other Hospitalizations and Active and Disabled Life Expectancy
Abstract
Importance: Estimates of active and disabled life expectancy, defined as the projected number of remaining years without and with disability in essential activities of daily living, are commonly used by policymakers to forecast the functional well-being of older persons.
Objective: To determine how estimates of active and disabled life expectancy differ based on exposure to intervening illnesses and injuries (or events).
Design, setting, and participants: This prospective cohort study was conducted in south-central Connecticut from March 1998 to December 2021 among 754 community-living persons aged 70 years or older who were not disabled. Data were analyzed from January 25 to September 18, 2024.
Exposures: Exposure to intervening events, which included critical illness, major elective and nonelective surgical procedures, and hospitalization for other reasons, was assessed each month.
Main outcomes and measures: Disability in 4 essential activities of daily living (bathing, dressing, walking, and transferring) was ascertained each month. Active and disabled life expectancy were estimated using multistate life tables under a discrete-time Markov process assumption.
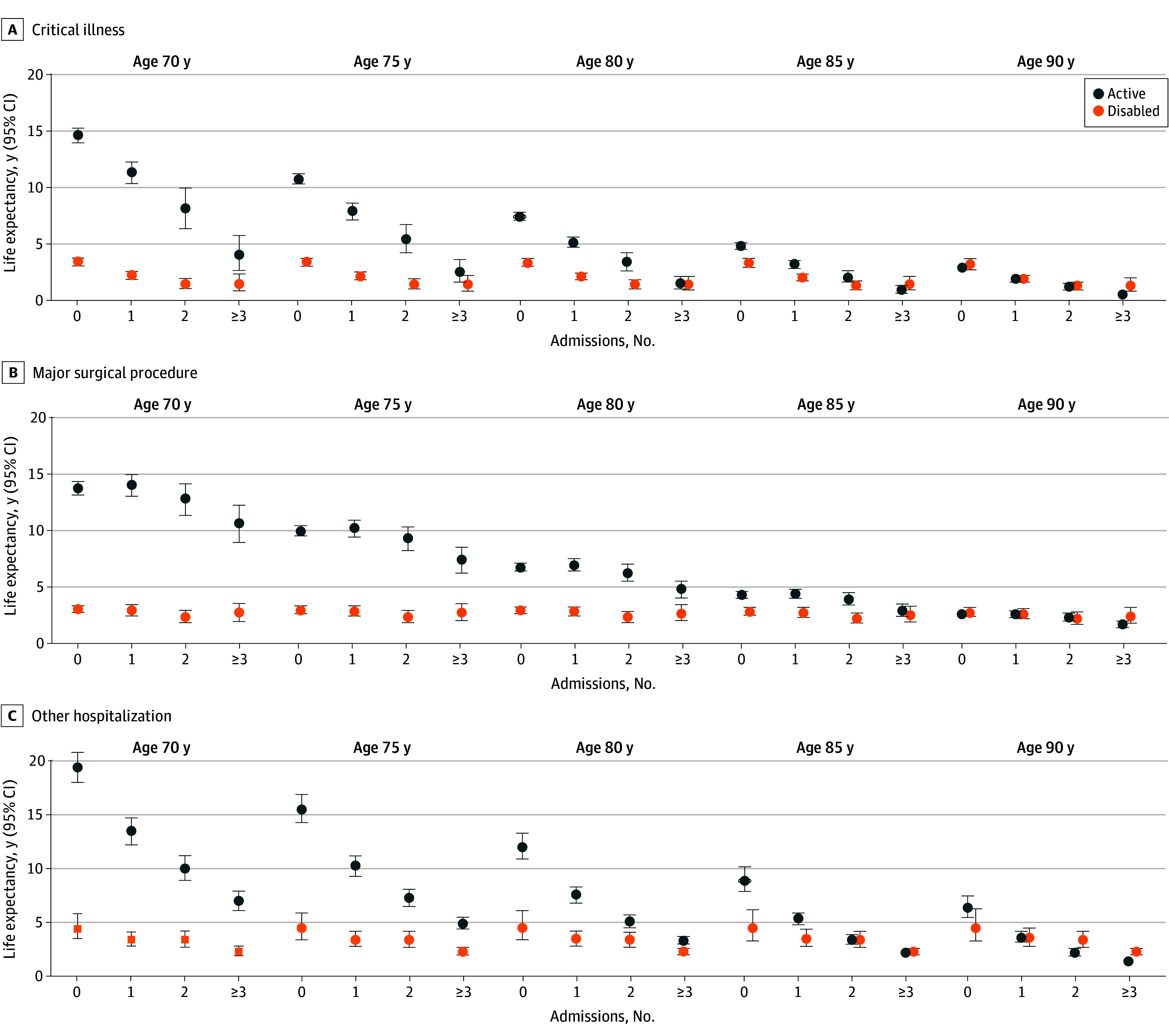
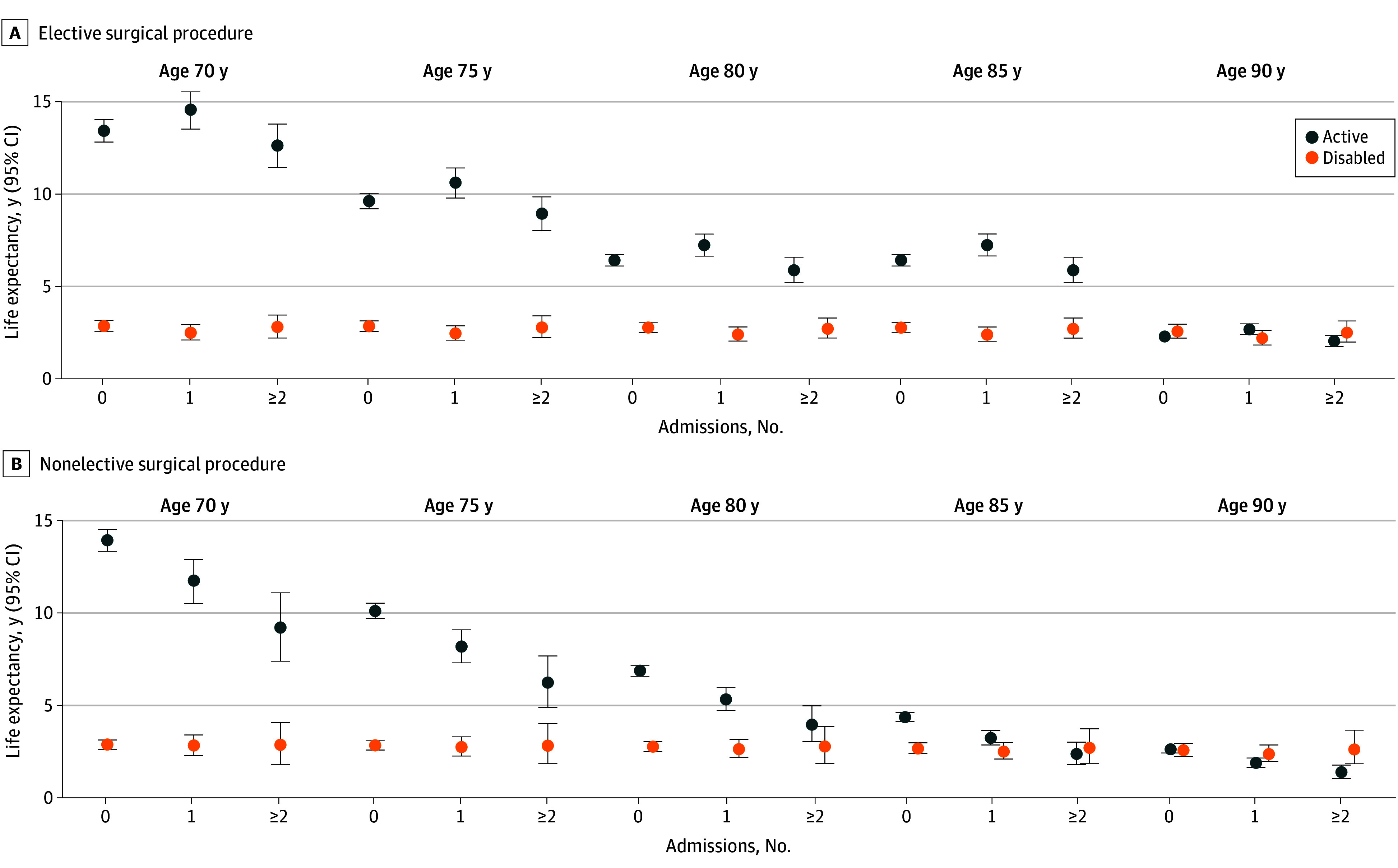
Results: The study included 754 community-living older persons who were not disabled (mean [SD] age, 78.4 [5.3] years; 487 female [64.6%]; 67 Black [8.9%], 4 Hispanic [0.5%], 682 non-Hispanic White [90.5%], and 1 other race [0.1%]). Within 5-year age increments from 70 to 90 years, active life expectancy decreased monotonically as the number of admissions for critical illness and other hospitalization increased. For example, at age 70 years, sex-adjusted active life expectancy decreased from 14.6 years (95% CI, 13.9-15.2 years) in the absence of a critical illness admission to 11.3 years (95% CI, 10.3-12.2 years), 8.1 years (95% CI, 6.3-9.9 years), and 4.0 years (95% CI, 2.6-5.7 years) in the setting of 1, 2, or 3 or more critical illness admissions, respectively. Corresponding values for other hospitalization were 19.4 years (95% CI, 18.0-20.8 years), 13.5 years (95% CI, 12.2-14.7 years), 10.0 years (95% CI, 8.9-11.2 years), and 7.0 years (95% CI, 6.1-7.9 years), respectively. Consistent monotonic reductions were observed for sex-adjusted estimates in active life expectancy for nonelective but not elective surgical procedures as the number of admissions increased; for example, at age 70 years, estimates of active life expectancy were 13.9 years (95% CI, 13.3-14.5 years), 11.7 years (95% CI, 10.5-12.8 years), and 9.2 years (95% CI, 7.4-11.0 years) for 0, 1, and 2 or more nonelective surgical admissions, respectively; corresponding values were 13.4 years (95% CI, 12.8-3-14.1 years), 14.6 years (95% CI, 13.5-15.5 years), and 12.6 years (95% CI, 11.5-13.8 years) for elective surgical admissions. Sex-adjusted disabled life expectancy decreased as the number of admissions increased for critical illness and other hospitalization but not for nonelective or elective surgical procedures; for example, at age 70 years, disabled life expectancy decreased from 4.4 years (95% CI, 3.5-5.8 years) in the absence of other hospitalization to 3.4 years (95% CI, 2.8-4.1 years), 3.4 years (95% CI, 2.7-4.2 years), and 2.3 years (95% CI, 1.9-2.8 years) in the setting of 1, 2, or 3 or more other hospitalizations, respectively.
Conclusions and relevance: This study found that active life expectancy among community-living older persons who were not disabled was considerably diminished in the setting of serious intervening illnesses and injuries. These findings suggest that prevention and more aggressive management of these events, together with restorative interventions, may be associated with improved functional well-being among older persons.
Conflict of interest statement
Figures
Similar articles
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
Association Between Restricting Symptoms and Disability After Critical Illness Among Older Adults.Crit Care Med. 2024 Dec 1;52(12):1816-1827. doi: 10.1097/CCM.0000000000006427. Epub 2024 Sep 18. Crit Care Med. 2024. PMID: 39298623 Free PMC article.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
