

The Lancet Commission on rethinking coronary artery disease: moving from ischaemia to atheroma
- PMID: 40179933
- PMCID: PMC12315672
- DOI: 10.1016/S0140-6736(25)00055-8
The Lancet Commission on rethinking coronary artery disease: moving from ischaemia to atheroma
Abstract
Coronary artery disease has long been understood through the paradigm of epicardial coronary artery obstruction, causing myocardial ischaemia (a mismatch between myocardial blood supply and demand). However, this model, which focuses on diagnosing and managing coronary artery disease based on ischaemia and cardiovascular events, is flawed. By the time ischaemia manifests, it is often too late for optimal intervention, limiting the effectiveness of treatment options. Despite decades of medical advances, coronary artery disease continues to be a leading cause of morbidity and mortality globally, highlighting the inadequacy of this traditional ischaemic-centric approach.
The central limitation of current approaches is the focus on the temporary solutions of restoring myocardial blood flow after obstruction, rather than tackling the underlying disease. Coronary artery disease, caused by atherosclerosis, often results in myocardial infarction through mechanisms that emerge earlier in the progression of disease. The focus of medical care has predominantly been on the recognition of symptoms and treatment of acute events, missing opportunities for early detection and prevention of disease. Billions of dollars in health-care funding continue to be spent on identifying and managing coronary ischaemia; yet, the dominant mechanisms for myocardial infarction are atherosclerotic plaque rupture or erosion and, to a lesser extent, erupted calcified nodules that can emerge at a much earlier stage of the disease.
This Commission advocates for a shift in the conceptual framework of coronary artery disease. We suggest reclassifying the condition as atherosclerotic coronary artery disease (ACAD), moving away from the traditional emphasis on ischaemia and acute cardiac events towards a more systematic understanding of atherosclerosis. This reframing will enable the identification and management of the disease much earlier in its course, potentially saving millions of lives worldwide.
Risk of ACAD develops over a lifetime, beginning in utero, progressing through childhood and adolescence, and continuing into older age. The early stages of disease, which involve the formation of atherosclerotic plaques, are often undetected. A major shift is needed from acute event-centred care to strategies focused on early diagnosis, prevention, and management of atherosclerosis. In this new framework, ACAD should be recognised across all stages, from the earliest signs of atheroma formation to the advanced stages of disease. Our goals should not just to be to manage symptoms and events but to prevent the disease from developing in the first place and, where possible, reverse its course.
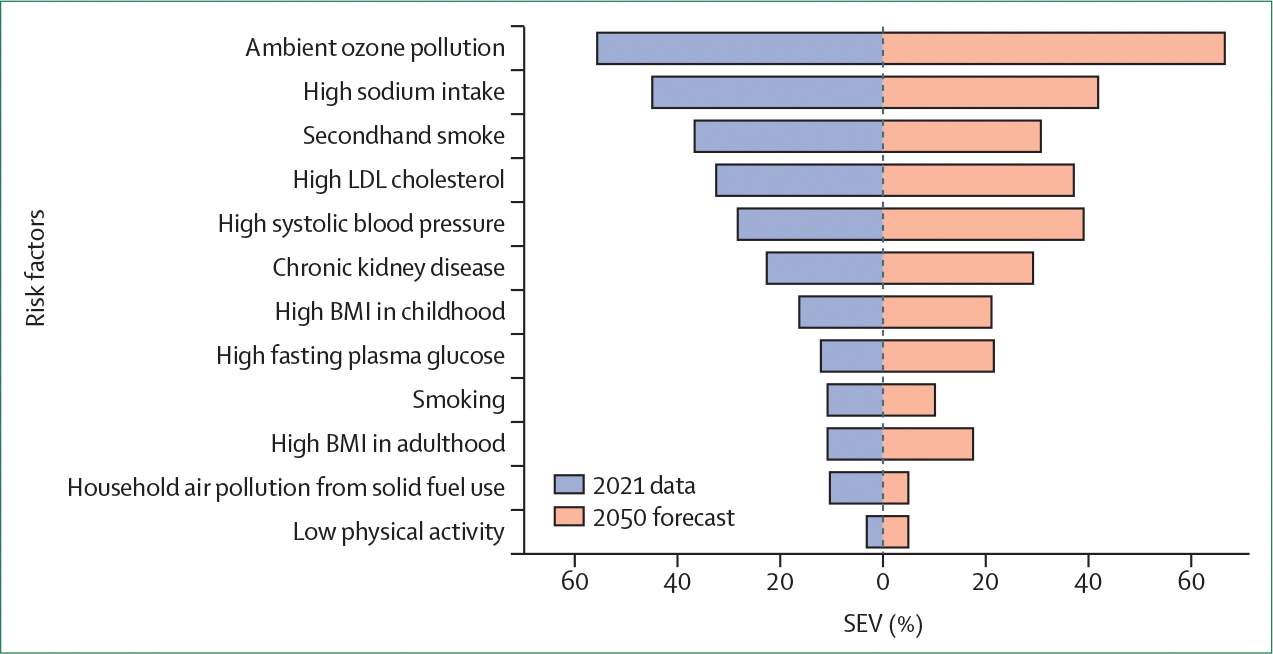
Early detection and prevention of ACAD: The prevention of ACAD must begin with early detection and modification of risk factors. If behavioural and metabolic risk factors, such as smoking, hypertension, high cholesterol, and poor diet, were eliminated or controlled early in life, the global burden of ACAD could be dramatically reduced. Eliminating these risk factors by 2050 could decrease the rate of ACAD deaths by 82·1%, potentially saving 8·7 million lives annually. Public health initiatives should emphasise lifestyle changes and the management of metabolic disorders to prevent the onset of atherosclerosis.
Early detection and effective prevention remain a challenge. The implementation of screening strategies to identify individuals at risk of developing ACAD is crucial. Targeted screening programmes, integrated into health-care systems, can detect early signs of atherosclerosis and enable timely intervention. Such interventions, if applied early, have the potential to halt, delay, or even reverse the progress of the disease, reducing the risk of cardiovascular events in later life.
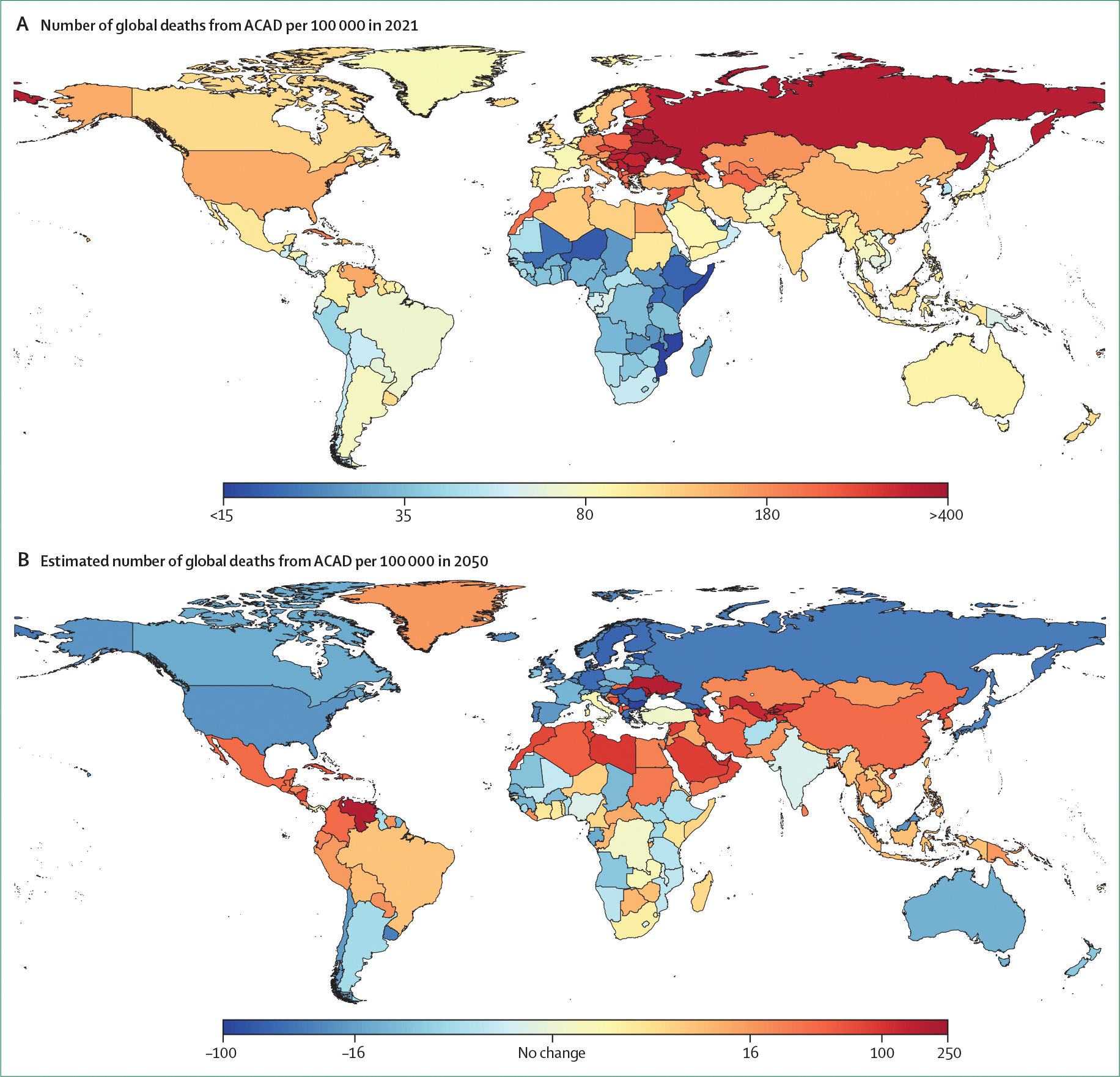
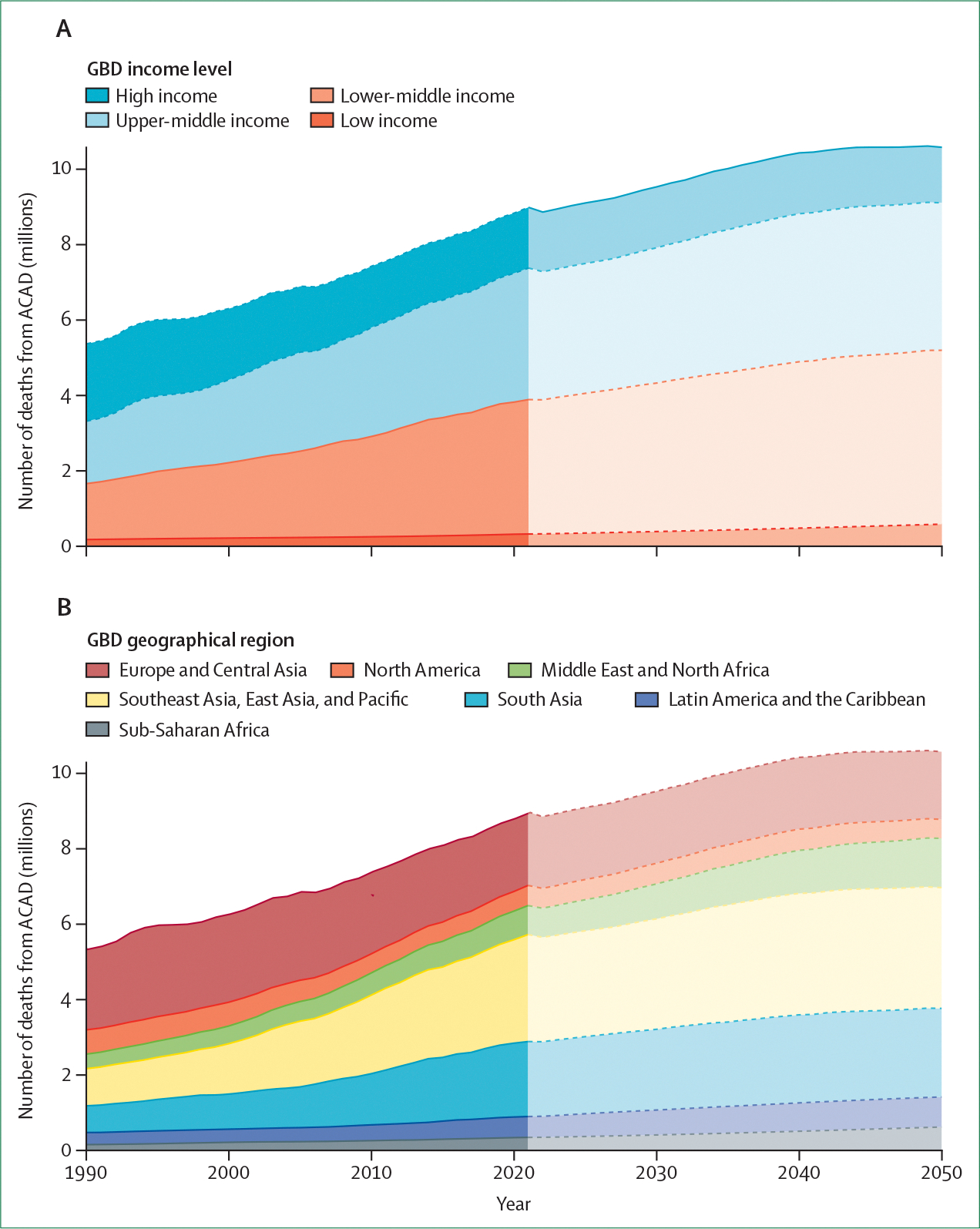
Addressing the global burden of ACAD: ACAD is not a uniform problem across the globe. Disparities exist between high-income countries and low-income to middle-income countries in terms of prevention, diagnosis, and treatment. These differences contribute to variations in health outcomes. Between 2022 and 2050, mortality rates from ACAD are forecasted to increase by 19·2% in lower-middle-income countries and 4·2% in upper-middle-income countries. This global disparity underscores the importance of equitable access to prevention, diagnosis, and treatment to reduce the global burden of ACAD.
Health-care systems must be designed to prioritise prevention and early detection of ACAD rather than simply treating advanced disease. This prioritisation requires a fundamental shift in the education and training of health-care providers, with a focus on the early stages of the disease and the integration of prevention strategies into clinical practice.
A comprehensive international approach to ACAD treatment requires increased research funding, the development of novel treatments, and investment in early detection methods. The development of new therapies to prevent, reverse, and eradicate atherosclerosis is crucial. Research funding must be increased to support these efforts, particularly in the development of transformative therapies and imaging technologies that can accurately assess disease progression at all stages.
Current research is insufficient and does not match the global burden of the disease. Research is not representative of diverse populations, often neglecting the specific needs of low-income and middle-income countries. More research is needed to ensure that clinical pathways for the prevention and treatment of ACAD are adaptable and effective across all health-care settings.
The reframing of coronary artery disease as ACAD represents a crucial shift in the way we approach the disease. By recognising ACAD as a lifelong condition, from early atherosclerotic plaques to advanced disease, and shifting priority towards early detection, prevention, and treatment, the potential to save millions of lives annually is substantial. Implementing these changes will require global collaboration, increased investment, and a commitment to equitable health-care delivery. Stakeholders should work together towards the stabilisation, reversal, and ultimate elimination of ACAD, reducing the global burden of this preventable disease.
Conflict of interest statement
Declaration of interests SZ reports grants from Abbott Vascular and personal fees from Novartis and Boston Scientific. JHW reports grants from the American Heart Association and National Institutes of Health; consulting fees from the Institute for Clinical and Economic Review, Pfizer, and Patient Centered Outcomes Research Institute; personal fees from Huff Powell Bailey; support for attending meetings and travel from the American College of Cardiology; and has a leadership and fiduciary role with the New England Comparative Effectiveness Public Affairs Council. VK reports support from Queen Mary University. BZ reports support from the David Geffen School of Medicine and VA Greater Los Angeles Healthcare System; grants from the National Institutes of Health, Veterans Administration, and American Heart Association; and personal fees from the Heart Failure Society of America, Circulation: Cardiovascular Quality and Outcomes, and Scholars in Medicine. WAP reports a leadership and fiduciary role within the Cardiac Society of Australia and New Zealand. TJAC reports support for attending meetings and travel from the University of Sheffield, British Heart Foundation Data Science Centre, and the estate of Mrs Reena Dyer. DCa reports consulting fees from Abbott Vascular; personal fees from Terumo, Sanofi Aventis, NovoNordisk, and Medtronic; and board participation for MedAlliance. NRS reports support for attending meetings and travel from Vanderbilt University Medical Center (for the submitted work); support from Society for Cardiovascular Angiography and Interventions and Zoll (outside the submitted work); grants from the National Institutes of Health, Society for Cardiovascular Angiography and Interventions, and Shockwave; personal fees from Philips, Abbott, Zoll, and Youman & Caputo; has a leadership role with the Women in Innovations Committee and the Society for Cardiovascular Angiography and Interventions; has stock options in Stallion Catheter; and stipend for serving as an associate editor for the Journal of the American Heart Association. RS reports grants from the National Institute for Health and Care Research and participation on a board for the UK Longitudinal Linkage Consortium. DCh reports personal fees from SpectraWave Medical Imaging. NG reports grant support from Abbott; personal fees from Abbott, ShockWave, Abiomed, Philips, and Boston Scientific; board participation for Boston Scientific and Abbott; and a leadership role with the European Association of Percutaneous Cardiovascular Interventions Scientific Documents Committee. SRM reports grant support from Abbott; personal fees from Amgen, Bristol Myers Squibb, Novartis, NovoNordisk, and Janssen; and board participation for Merck. JS reports stock in Anagram Kommunikation and Symptoms Europe. SJN reports grants from AstraZeneca, Amgen, Anthera, CSL Behring, Cerenis, Cyclarity, Eli Lilly, Esperion, Resverlogix, New Amsterdam Pharma, Novartis, InfraReDx, and Sanofi-Regeneron; personal fees from Amgen, Akcea, AstraZeneca, Boehringer Ingelheim, CSL Behring, Eli Lilly, Esperion, Kowa, Merck, Takeda, Pfizer, Sanofi-Regeneron, Vaxxinity, Sequiris, and NovoNordisk; is listed as inventor on the patent for effects of PCSK9 inhibition on coronary atherosclerosis; has a leadership and fiduciary role with Cardiac Society of Australia and New Zealand; and is director of Evidence to Practice (non-profit meeting company). LJS reports a leadership and fiduciary role with the Society of Cardiovascular Computed Tomography and that HeartFlow granted access to their software. MRP reports grants from HeartFlow, Johnson & Johnson, National Heart, Lung and Blood Institute, and Patient Centered Outcomes Research Institute and personal fees from Bayer Healthcare, Janssen, Novartis, and Medscape. RKA-L reports grant support from the British Heart Foundation; personal fees from Abbott Vascular, Fondazione Internazionale Menarini, Shockwave, Cathworks, Medtronic, Philips, and Servier Pharmaceuticals; and board participation for Janssen Pharmaceuticals and Cathworks. All other authors declare no competing interests.
Figures









References
-
- Silverman ME. William Herberden and some account of a disorder of the breast. Clin Cariol 1987; 10: 211–13. - PubMed
-
- Hektoen L. Embolism of the left coronary artery; sudden death. Med Newsl 1892; 61: 210.
-
- Obrastzov WP, Straschesko ND. Zur Kenntnis der Thrombose der Koronararterien des Herzens. Z Klin Med 1910; 71: 116–32.
-
- Herrick JB. Certain clinical features of sudden obstruction of the coronary arteries. J Am Med Assoc 1912; 59: 2015–20.
-
- Goetz RH, Rohman M, Haller JD, Dee R, Rosenak SS. Internal mammary-coronary artery anastomosis—a nonsuture method employing tantalum rings. J Thorac Cardiovasc Surg 1961; 41: 378–86. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
