

Tissue Adequacy and Diagnostic Yield Assessment in Malignant Lymph Nodes Using Endobronchial Ultrasound (EBUS)-Guided Miniforcep Biopsy vs. EBUS-Guided Transbronchial Needle Aspiration
- PMID: 40179948
- PMCID: PMC12235285
- DOI: 10.4046/trd.2024.0134
Tissue Adequacy and Diagnostic Yield Assessment in Malignant Lymph Nodes Using Endobronchial Ultrasound (EBUS)-Guided Miniforcep Biopsy vs. EBUS-Guided Transbronchial Needle Aspiration
Abstract
Background: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a predominantly used method for lymph node (LN) metastasis assessment. This study aims to identify tissue adequacy improvement with the addition of EBUS-guided miniforcep biopsy (EBUS-MFB) to EBUS-TBNA in sampling LNs.
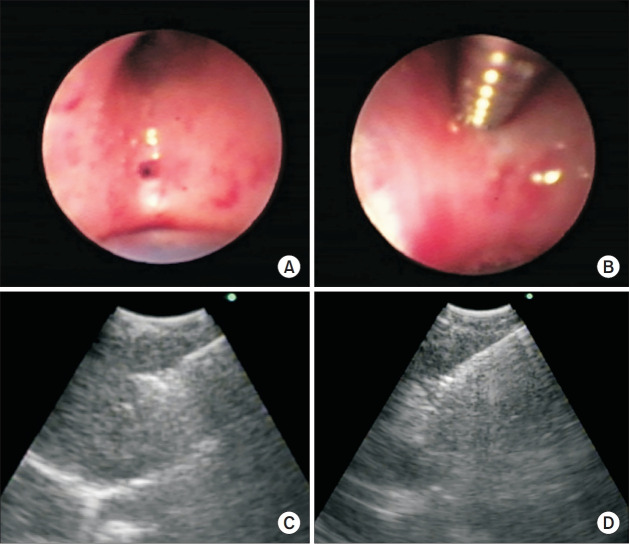
Methods: We assessed tissue adequacy in patients with mediastinal and hilar lymphadenopathy, comparing the combination of EBUS-MFB and EBUS-TBNA with EBUS-TBNA alone. EBUS-MFB was performed with the guide sheath (GS) dilatation technique. Tissue adequacy was a tumor cell count (TCC) of >100 and neoplastic cell neoplastic cell estimate of >25%. Further, we reported the diagnostic yield, tumor cell characteristics, and safety outcomes.
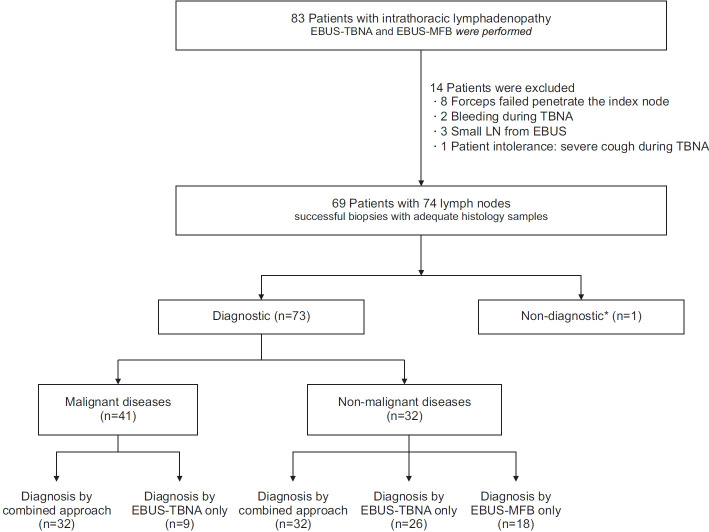
Results: Among 69 patients (74 nodes), malignant diseases were diagnosed in 41 nodes using both techniques. Tissue adequacy with EBUS-TBNA (93.8% in 30/32 nodes) was comparable with the combined group (96.9% in 31/32 nodes, p=0.317). EBUS-TBNA yielded higher TCC (84.4% with >1,000 cells) than EBUS-MFB (53.1%, p=0.004). The combined approach significantly improved the diagnostic yield in non-malignant diseases compared with EBUS-TBNA alone (97% vs. 78.8%, p=0.014). Of the 32 nodes, 20 demonstrated discordant results between EBUS-TBNA and EBUS-MFB, with EBUS-MFB correctly diagnosing six nodes that EBUS-TBNA misdiagnosed. The complication rate was low (2.9%) with only minor bleeding reported.
Conclusion: EBUS-TBNA alone and the combination of EBUS-MFB and EBUS-TBNA demonstrated comparable tissue adequacy, with EBUS-TBNA exhibiting better specimen characteristics, potentially sufficient for various molecular analyses. The addition of EBUS-MFB, performed using the GS-dilatation technique, to EBUS-TBNA improved the diagnostic yield and proved to be a safe and efficient approach, particularly in non-malignant diseases.
Keywords: Endobronchial Ultrasound; Mediastinal and Hilar Lymphadenopathy; Miniforcep Biopsy; Tissue Adequacy; Transbronchial Needle Aspiration.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Is the diagnostic yield of mediastinal lymph node cryobiopsy (cryoEBUS) better for diagnosing mediastinal node involvement compared to endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA)? A systematic review.Respir Med. 2023 Nov;218:107389. doi: 10.1016/j.rmed.2023.107389. Epub 2023 Aug 12. Respir Med. 2023. PMID: 37579981
-
Utility and Safety of Endoscopic Ultrasound With Bronchoscope-Guided Fine-Needle Aspiration in Mediastinal Lymph Node Sampling: Systematic Review and Meta-Analysis.Respir Care. 2015 Jul;60(7):1040-50. doi: 10.4187/respcare.03779. Epub 2015 Mar 10. Respir Care. 2015. PMID: 25759463
-
Diagnostic Value of Convex Probe Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration in Mediastinal Tuberculous Lymphadenitis: A Systematic Review and Meta-Analysis.Med Sci Monit. 2015 Jul 16;21:2064-72. doi: 10.12659/MSM.894526. Med Sci Monit. 2015. PMID: 26177653 Free PMC article.
-
Mediastinal restaging in non-small cell lung cancer: comparing endobronchial ultrasound-guided transbronchial needle aspiration and mediastinal cryobiopsy following neoadjuvant therapy.Mediastinum. 2025 Jun 25;9:11. doi: 10.21037/med-25-11. eCollection 2025. Mediastinum. 2025. PMID: 40666530 Free PMC article.
-
Endobronchial ultrasound-guided transbronchial needle aspiration in real-life settings.Respir Med. 2025 Sep;246:108239. doi: 10.1016/j.rmed.2025.108239. Epub 2025 Jul 1. Respir Med. 2025. PMID: 40609702
References
-
- Wang KP. Flexible transbronchial needle aspiration biopsy for histologic specimens. Chest. 1985;88:860–3. - PubMed
-
- Chrissian A, Misselhorn D, Chen A. Endobronchial-ultrasound guided miniforceps biopsy of mediastinal and hilar lesions. Ann Thorac Surg. 2011;92:284–8. - PubMed
-
- Franke KJ, Bruckner C, Szyrach M, Ruhle KH, Nilius G, Theegarten D. The contribution of endobronchial ultrasound-guided forceps biopsy in the diagnostic workup of unexplained mediastinal and hilar lymphadenopathy. Lung. 2012;190:227–32. - PubMed
-
- Darwiche K, Freitag L, Nair A, Neumann C, Karpf-Wissel R, Welter S, et al. Evaluation of a novel endobronchial ultrasound-guided lymph node forceps in enlarged mediastinal lymph nodes. Respiration. 2013;86:229–36. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
