

Formyl-peptide receptor type 2 activation mitigates heart and lung damage in inflammatory arthritis
- PMID: 40181186
- PMCID: PMC12081931
- DOI: 10.1038/s44321-025-00227-1
Formyl-peptide receptor type 2 activation mitigates heart and lung damage in inflammatory arthritis
Abstract
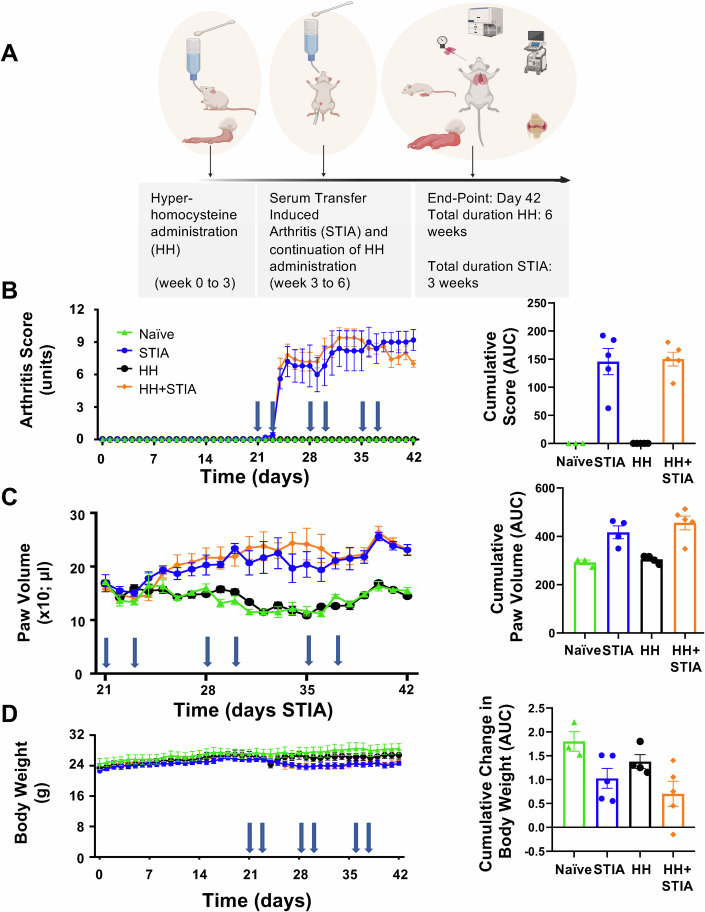
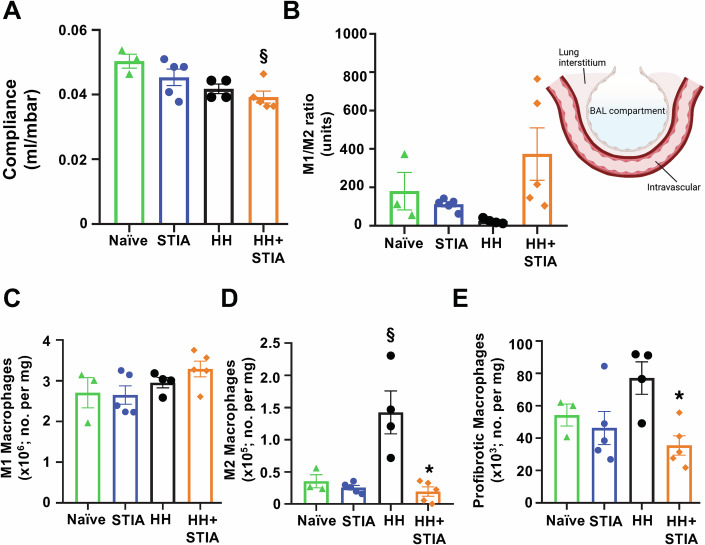
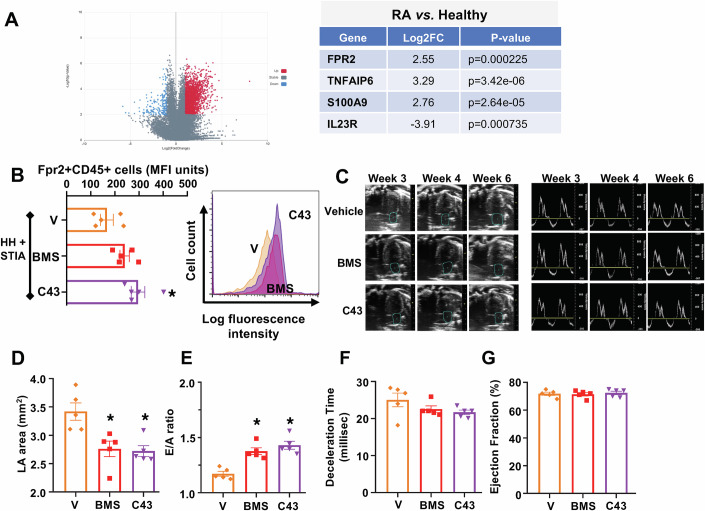
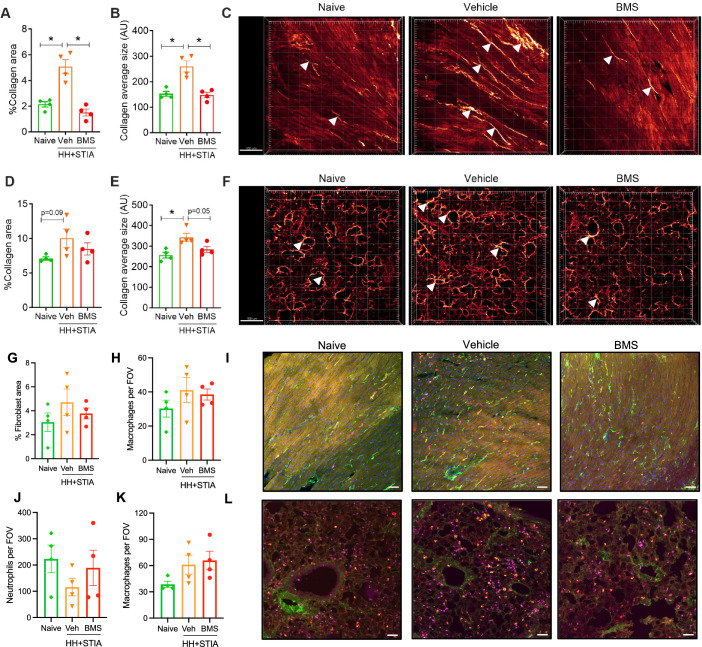
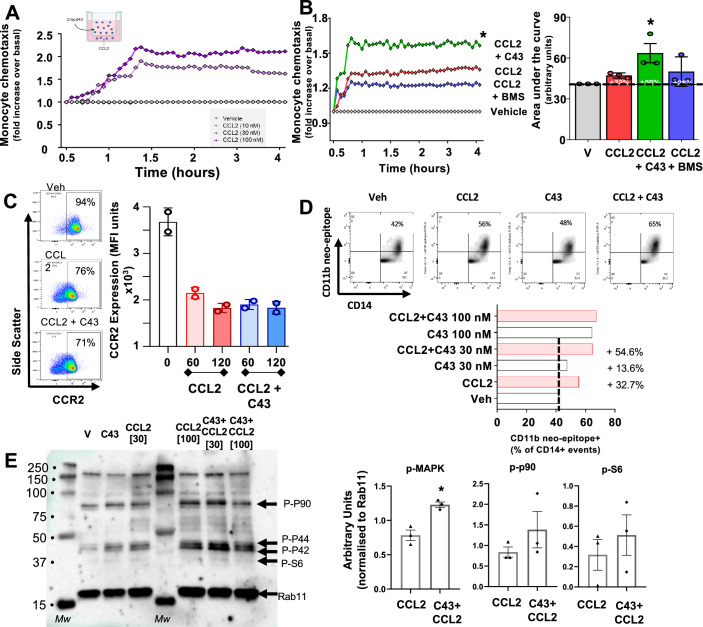
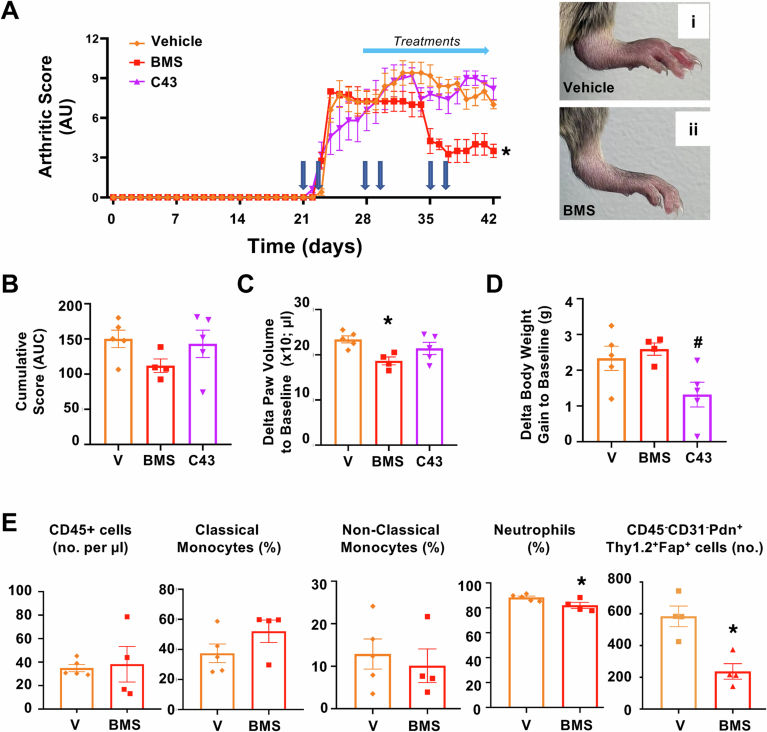
Rheumatoid arthritis (RA) is associated with heart and lung dysfunction. Current therapies fail to attenuate such complications. Here, we identify formyl-peptide receptor type 2 (FPR2) as a therapeutic target to treat heart and lung dysfunction associated with inflammatory arthritis. Arthritic mice on high levels of dietary homocysteine develop cardiac diastolic dysfunction and reduced lung compliance, mirroring two comorbidities in RA. Therapeutic administration of a small molecule FPR2 agonist (BMS986235) to hyper-homocysteine arthritic mice prevented diastolic dysfunction (monitored by echocardiography) and restored lung compliance. These tissue-specific effects were secondary to reduced neutrophil infiltration, modulation of fibroblast activation and phenotype (in the heart) and attenuation of monocyte and macrophage numbers (in the lung). A dual FPR1/2 agonist (compound 43) failed to prevent the reduction in lung compliance of arthritic mice and promoted the accumulation of inflammatory monocytes and pro-fibrotic macrophages in lung parenchyma. This cellular response lies downstream of FPR1-mediated potentiation of CCL2-dependent monocyte chemotaxis and activation. This finding supports the therapeutic development of selective FPR2 agonists to mitigate two impactful comorbidities associated with inflammatory arthritides.
Keywords: HFpEF; Lung Injury; Pro-resolving GPCR; Resolution Pharmacology; Rheumatoid Arthritis.
© 2025. The Author(s).
Conflict of interest statement
Disclosure and competing interests statement. MP declares to be a shareholder of ResoTher Pharma ApS and a director of William Harvey Research Limited; advisory board member for SynAct Pharma AB; and is involved in the following commercial projects: SynAct Pharma AB and TXP Pharma AG. MP and JD are inventors on a patent related to AnxA1 pro-resolving peptides (European Patent 3533457 B1). JAL, NRW and RAG are employees of Bristol Myers Squibb and hold shares in the company.
Figures







Similar articles
-
Discovery of BMS-986235/LAR-1219: A Potent Formyl Peptide Receptor 2 (FPR2) Selective Agonist for the Prevention of Heart Failure.J Med Chem. 2020 Sep 10;63(17):9003-9019. doi: 10.1021/acs.jmedchem.9b02101. Epub 2020 May 24. J Med Chem. 2020. PMID: 32407089
-
Small-molecule-biased formyl peptide receptor agonist compound 17b protects against myocardial ischaemia-reperfusion injury in mice.Nat Commun. 2017 Feb 7;8:14232. doi: 10.1038/ncomms14232. Nat Commun. 2017. PMID: 28169296 Free PMC article.
-
A formyl peptide receptor agonist suppresses inflammation and bone damage in arthritis.Br J Pharmacol. 2014 Sep;171(17):4087-96. doi: 10.1111/bph.12768. Br J Pharmacol. 2014. PMID: 24824742 Free PMC article.
-
Recent advances in the design and development of formyl peptide receptor 2 (FPR2/ALX) agonists as pro-resolving agents with diverse therapeutic potential.Eur J Med Chem. 2021 Mar 5;213:113167. doi: 10.1016/j.ejmech.2021.113167. Epub 2021 Jan 12. Eur J Med Chem. 2021. PMID: 33486199 Review.
-
Treating neutrophilic inflammation in COPD by targeting ALX/FPR2 resolution pathways.Pharmacol Ther. 2013 Dec;140(3):280-9. doi: 10.1016/j.pharmthera.2013.07.007. Epub 2013 Jul 21. Pharmacol Ther. 2013. PMID: 23880288 Review.
Cited by
-
Getting to the heart of cardiovascular complications associated with inflammatory arthritis.EMBO Mol Med. 2025 May;17(5):869-871. doi: 10.1038/s44321-025-00226-2. Epub 2025 Apr 3. EMBO Mol Med. 2025. PMID: 40181185 Free PMC article.
-
Immunogenic cell death-related biomarkers in heart failure probed by transcriptome and single-cell sequencing.Front Immunol. 2025 Jun 24;16:1560903. doi: 10.3389/fimmu.2025.1560903. eCollection 2025. Front Immunol. 2025. PMID: 40630963 Free PMC article.
References
-
- Abdulrahman N, Jaballah M, Poomakkoth N, Riaz S, Abdelaziz S, Issa A, Mraiche F (2016) Inhibition of p90 ribosomal S6 kinase attenuates cell migration and proliferation of the human lung adenocarcinoma through phospho-GSK-3beta and osteopontin. Mol Cell Biochem 418:21–29 - PubMed
-
- Asahina Y, Wurtz NR, Arakawa K, Carson N, Fujii K, Fukuchi K, Garcia R, Hsu MY, Ishiyama J, Ito B et al (2020) Discovery of BMS-986235/LAR-1219: a potent formyl peptide receptor 2 (FPR2) selective agonist for the prevention of heart failure. J Med Chem 63:9003–9019 - PubMed
-
- Binder MD, Fox AD, Merlo D, Johnson LJ, Giuffrida L, Calvert SE, Akkermann R, Ma GZM, ANZgene, Perera AA, Gresle MM, Laverick L, Foo G, Fabis-Pedrini MJ, Spelman T, Jordan MA, Baxter AG, Foote S, Butzkueven H, Kilpatrick TJ, Field J (2016) Common and Low Frequency Variants in MERTK Are Independently Associated with Multiple Sclerosis Susceptibility with Discordant Association Dependent upon HLA-DRB1*15:01 Status. PLoS Genet. 12:e1005853 - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
