

Ketamine as part of multi-modal analgesia may reduce opioid requirements following cardiac surgery: a retrospective observational cohort study
- PMID: 40181432
- PMCID: PMC11966800
- DOI: 10.1186/s13019-025-03405-x
Ketamine as part of multi-modal analgesia may reduce opioid requirements following cardiac surgery: a retrospective observational cohort study
Abstract
Background: Postoperative pain control in cardiac surgery is often managed with opioid medications. Insufficient analgesia can result in complications including splinting, pneumonia, and delay of appropriate rehabilitation. Given the risks and adverse effects of opioids including sedation, respiratory depression, delirium, and decreased gastrointestinal motility, hyperalgesia and potential for addiction, strategies for opioid reduction are likely to improve outcomes, therefore multimodal opioid sparing pain regimens are preferred. Recently, there is increased evidence that low dose Ketamine, an N-methyl-D-Aspartate (NMDA) receptor antagonist, is safe and effective for analgesia in postoperative patients and may be appropriate to this setting.
Methods: This is a single center, retrospective, observational, cohort study over a one year period involving postoperative adult cardiac surgery comparing those who received a single dose of postoperative ketamine, 0.3 mg/kg over 30 min, with those who did not receive any ketamine. Other analgesic protocols were similar between groups and did not include additional ketamine. A total of 120 patient charts were reviewed, of which 96 met inclusion criteria, 32 in the ketamine group and 64 in the standard care group. Charts were reviewed for opioid and other pain medication requirements during the postoperative period and on discharge, and for secondary outcomes: hospital length of stay, ICU length of stay, in-hospital and 30-day mortality, 30-day readmission, and rates of delirium, emergence reactions, and need for escalated respiratory support.
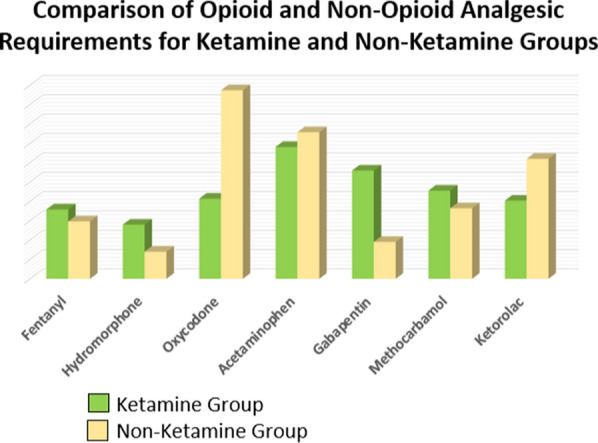
Results: The group who received postoperative ketamine required 28.8 morphine milligram equivalents (MME) less postoperative opioid (90.1 mg vs 118.9 mg, p = 0.167), and was prescribed an average of 15.8 MME less on discharge (p < 0.001). Intraoperatively, both groups received 1000 mg acetaminophen, 2 mg intravenous morphine and 100 mcg fentanyl, 26 MME, by protocol. No ketamine was administered intraoperatively or preoperatively. The groups differed in respect to operation type and controlling for this parameter failed to achieve significance in needs during admission (p = 0.215), but remained significant on discharge (p = 0.02). The non-ketamine group received more ketorolac (15.5 vs 10.1, p = 0.06). The ketamine group required less acetaminophen but more gabapentin. There was no difference in hospital or ICU length of stay. There was no delirium or mortality in either group. Respiratory depression occurred in 15 patients who all subsequently received ketamine. No patient developed respiratory depression after ketamine.
Conclusions: Ketamine may be a reasonable choice for postoperative cardiac surgery analgesia and may reduce the need for opioids on discharge, and possibly during admission.
Keywords: Ketamine; Multimodal analgesia; Opioid-sparing effect; Postoperative pain management.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics and approval and consent to participate: This trial was reviewed and approved by the institutional review board of New York University, reference number i24-00258. The board determined that this study, as a retrospective observational study without identifying protected health information, qualified for a waiver of consent. Consent for publication: There is no individual or identifying data in the study that would necessitate consent for publishing. Competing interests: The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
