

The preoperative flexion tear gap affects postoperative meniscus stability after pullout repair for medial meniscus posterior root tear
- PMID: 40181486
- PMCID: PMC11969855
- DOI: 10.1186/s43019-025-00264-7
The preoperative flexion tear gap affects postoperative meniscus stability after pullout repair for medial meniscus posterior root tear
Abstract
Background: We investigated whether the preoperative flexion tear gap (FTG) observed in open magnetic resonance imaging (MRI) affects meniscus stability after medial meniscus (MM) posterior root (MMPR) repairs. Furthermore, time-correlated MRI findings from MMPR tear occurrence were evaluated.
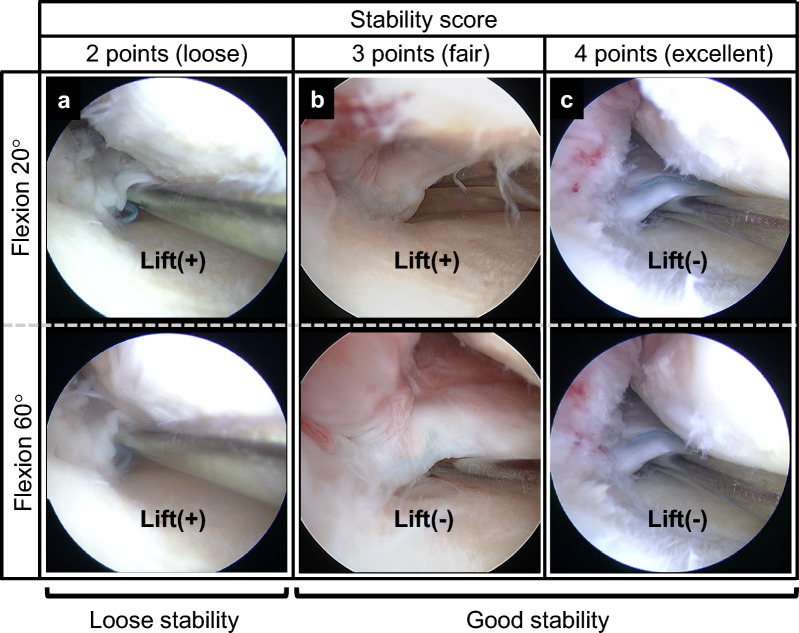
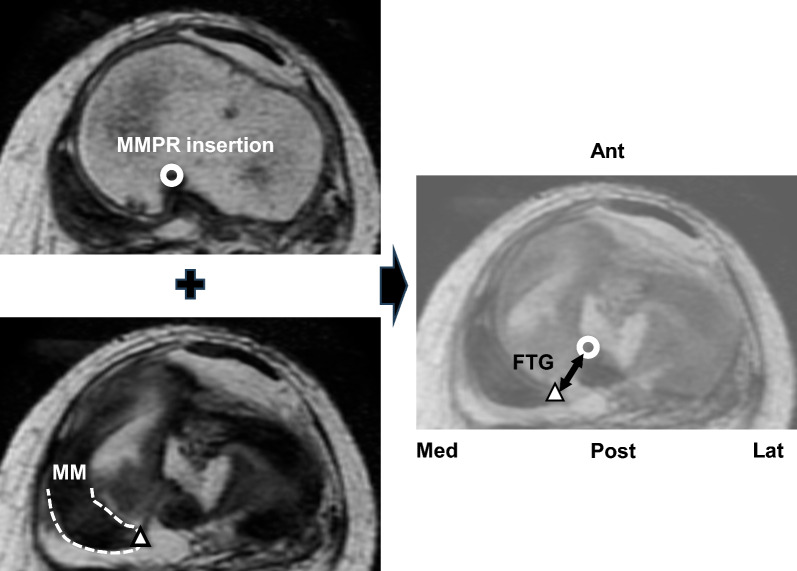
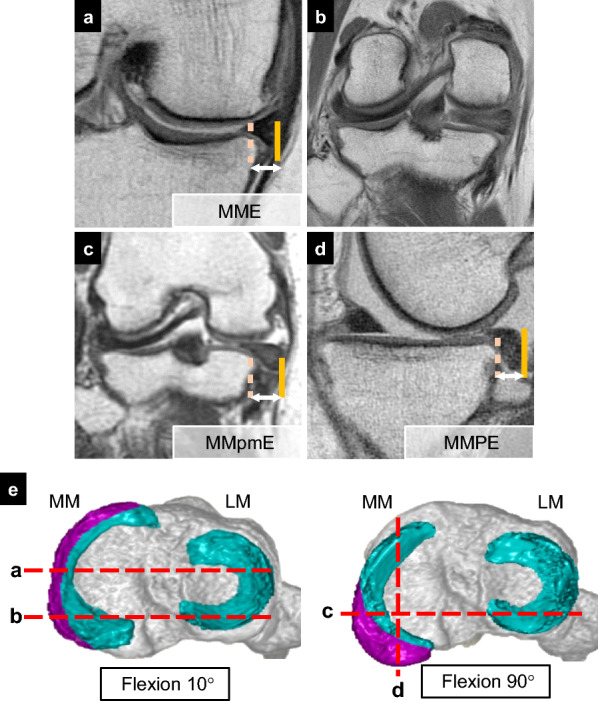
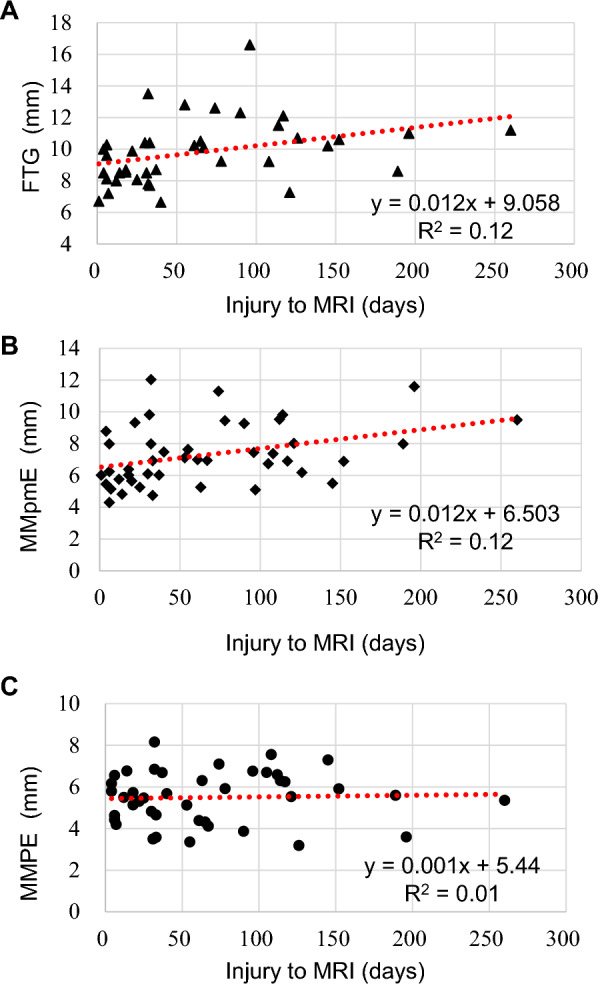
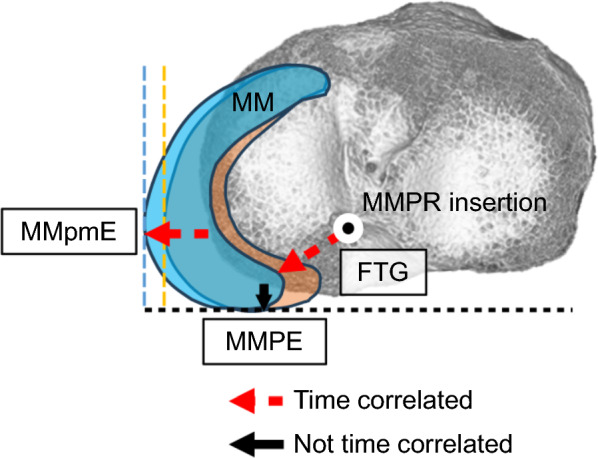
Methods: This retrospective observational study included 54 patients (mean age, 64.6 years; 13 males and 41 females) who underwent pullout repair for radial degenerative MMPR tear. Meniscus stability (scored 0-4 points) was assessed using a semi-quantitative arthroscopic scoring system during second-look arthroscopy 1 year postoperatively. The FTG was evaluated on preoperative axial MRI at 90° knee flexion. Other MRI measurements included MM extrusion (MME) at 10° knee flexion, MM posterior extrusion (MMPE) at 90° knee flexion, and MM posteromedial extrusion (MMpmE) at 90° knee flexion preoperatively and 1 year postoperatively. The correlation between the arthroscopic stability score and MRI findings was investigated. A receiver-operating characteristic curve was calculated to predict a good meniscus healing score (3-4 points). The correlation between the FTG and patient demographics, including time from injury to MRI, was analyzed.
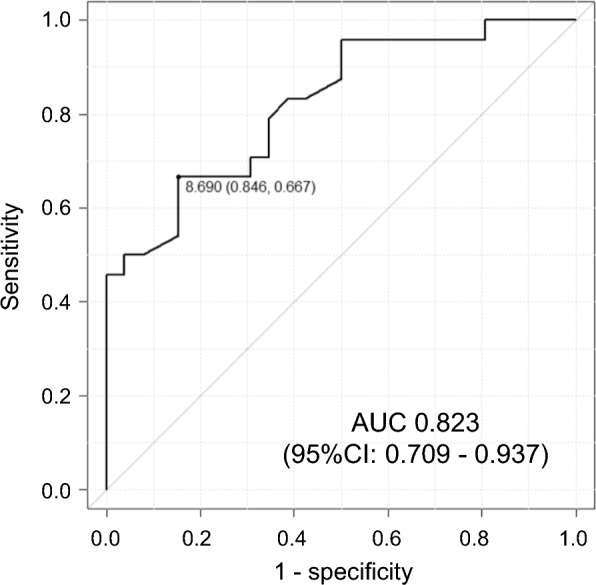
Results: At 1 year postoperatively, MME increased by 1.1 mm, while MMpmE and MMPE decreased by 0.4 mm and 1.0 mm, respectively. The meniscus stability score was negatively correlated with the preoperative FTG (r = -0.61, p < 0.01). The time from injury to MRI was significantly correlated with the preoperative FTG. The receiver-operating characteristic curve identified an FTG cut-off value of 8.7 mm for predicting good postoperative stability, with sensitivity and specificity of 67% and 85%, respectively.
Conclusions: FTG evaluated with open MRI at 90° knee flexion was associated with time from injury and affected meniscus stability following pullout repair. MMPR tears should be treated in the early phase to increase meniscus healing stability.
Keywords: Distance; Medial meniscus; Posterior root tear; Pullout repair; Second-look arthroscopy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Our hospital’s institutional review board approved this retrospective study (approval number: 1857), and all patients provided written informed consent. Consent for publication: Written informed consent was obtained from all study participants. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Placement of an anatomic tibial tunnel significantly improves the medial meniscus posterior extrusion at 90° of knee flexion following medial meniscus posterior root pullout repair.Knee Surg Sports Traumatol Arthrosc. 2021 Apr;29(4):1025-1034. doi: 10.1007/s00167-020-06070-w. Epub 2020 May 25. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32451621
-
Transtibial fixation for medial meniscus posterior root tear reduces posterior extrusion and physiological translation of the medial meniscus in middle-aged and elderly patients.Knee Surg Sports Traumatol Arthrosc. 2020 Nov;28(11):3416-3425. doi: 10.1007/s00167-019-05810-x. Epub 2019 Nov 28. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31781798
-
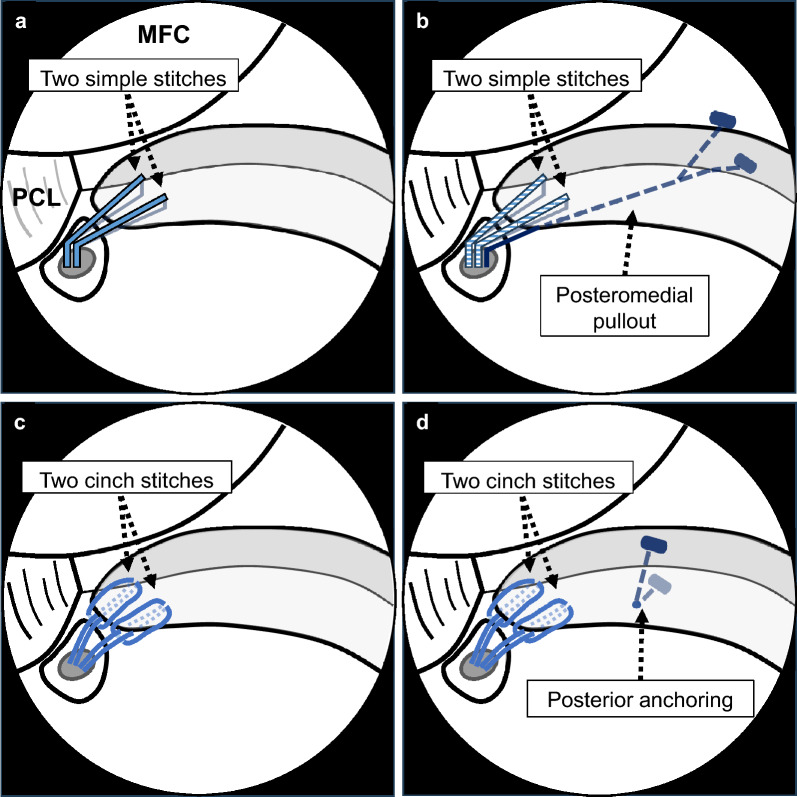
Comparison of two simple stitches and modified Mason-Allen suture for medial meniscus posterior root tear based on the progression of meniscal posterior extrusion: A retrospective cohort study.J Orthop Surg (Hong Kong). 2021 Sep-Dec;29(3):23094990211049569. doi: 10.1177/23094990211049569. J Orthop Surg (Hong Kong). 2021. PMID: 34775855
-
Lateral meniscus posterior root repairs show superior healing, reduced meniscal extrusion and improved clinical outcomes compared to medial meniscus posterior root repairs: A systematic review.Knee Surg Sports Traumatol Arthrosc. 2025 Feb;33(2):581-605. doi: 10.1002/ksa.12478. Epub 2024 Sep 26. Knee Surg Sports Traumatol Arthrosc. 2025. PMID: 39324377
-
Examining the Efficacy of Medial Meniscus Posterior Root Repair: A Meta-analysis and Systematic Review of Biomechanical and Clinical Outcomes.Am J Sports Med. 2023 Jun;51(7):1914-1926. doi: 10.1177/03635465221077271. Epub 2022 Apr 6. Am J Sports Med. 2023. PMID: 35384728
Cited by
-
Why Hoop Tension Matters: A Biomechanical Perspective on Medial Meniscus Posterior Root Tears-A Narrative Review.Bioengineering (Basel). 2025 Jun 11;12(6):638. doi: 10.3390/bioengineering12060638. Bioengineering (Basel). 2025. PMID: 40564454 Free PMC article. Review.
References
-
- Furumatsu T, Kamatsuki Y, Fujii M, Kodama Y, Okazaki Y, Masuda S, Ozaki T (2017) Medial meniscus extrusion correlates with disease duration of the sudden symptomatic medial meniscus posterior root tear. Orthop Traumatol Surg Res 103:1179–1182 - PubMed
-
- Moon HS, Choi CH, Jung M, Lee DY, Hong SP, Kim SH (2020) Early surgical repair of medial meniscus posterior root tear minimizes the progression of meniscal extrusion: 2-year follow-up of clinical and radiographic parameters after arthroscopic transtibial pull-out repair. Am J Sports Med 48:2692–2702 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
