

Evolution of Preclinical Models for Glioblastoma Modelling and Drug Screening
- PMID: 40183896
- PMCID: PMC12081544
- DOI: 10.1007/s11912-025-01672-4
Evolution of Preclinical Models for Glioblastoma Modelling and Drug Screening
Abstract
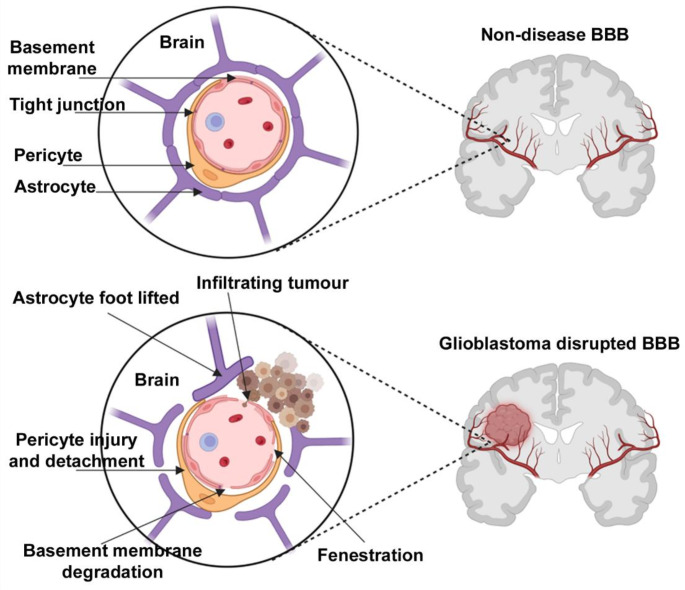
Purpose of review: Isocitrate dehydrogenase wild-type glioblastoma is an extremely aggressive and fatal primary brain tumour, characterised by extensive heterogeneity and diffuse infiltration of brain parenchyma. Despite multimodal treatment and diverse research efforts to develop novel therapies, there has been limited success in improving patient outcomes. Constructing physiologically relevant preclinical models is essential to optimising drug screening processes and identifying more effective treatments.
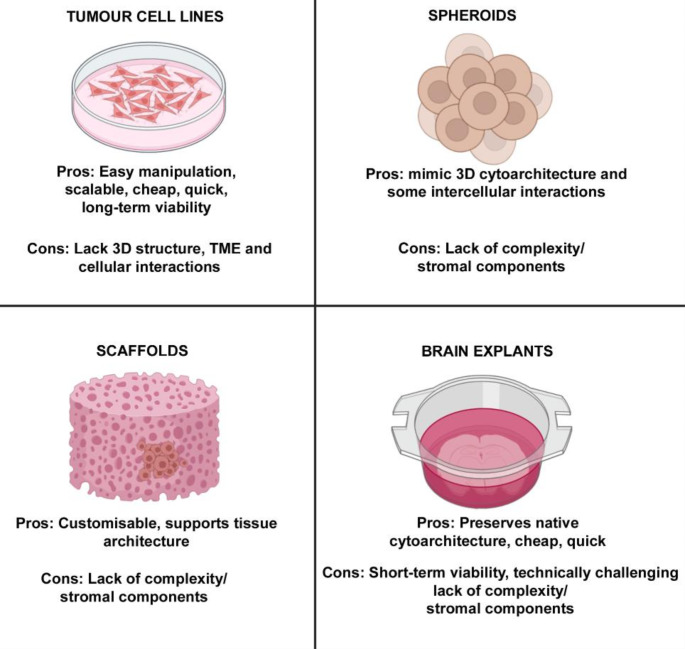
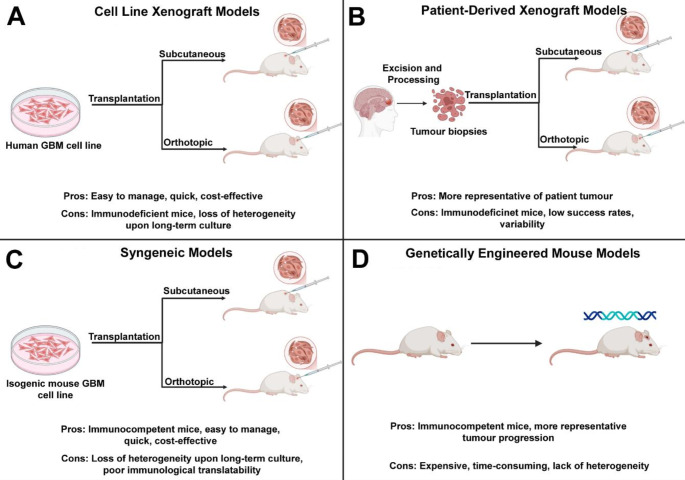
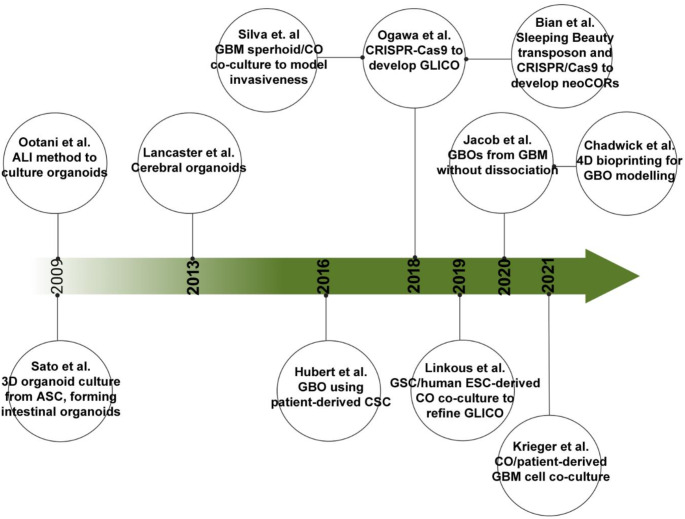
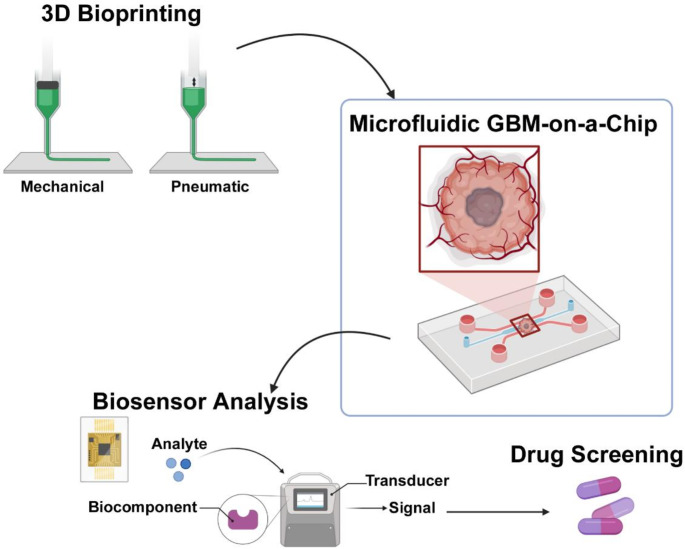
Recent findings: Traditional in-vitro models have provided critical insights into glioblastoma pathophysiology; however, they are limited in their ability to recapitulate the complex tumour microenvironment and its interactions with surrounding cells. In-vivo models offer a more physiologically relevant context, but often do not fully represent human pathology, are expensive, and time-consuming. These limitations have contributed to the low translational success of therapies from trials to clinic. Organoid and glioblastoma-on-a-chip technology represent significant advances in glioblastoma modelling and enable the replication of key features of the human tumour microenvironment, including its structural, mechanical, and biochemical properties. Organoids provide a 3D system that captures cellular heterogeneity and tumour architecture, while microfluidic chips offer dynamic systems capable of mimicking vascularisation and nutrient exchange. Together, these technologies hold tremendous potential for high throughput drug screening and personalised, precision medicine. This review explores the evolution of preclinical models in glioblastoma modelling and drug screening, emphasising the transition from traditional systems to more advanced organoid and microfluidic platforms. Furthermore, it aims to evaluate the advantages and limitations of both traditional and next-generation models, investigating their combined potential to address current challenges by integrating complementary aspects of specific models and techniques.
Keywords: Glioblastoma; Glioblastoma-on-a-chip; Microfluids; Organoids; Preclinical model.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing Interests: The authors declare no competing interests.
Figures
Similar articles
-
Microengineered 3D Tumor Models for Anti-Cancer Drug Discovery in Female-Related Cancers.Ann Biomed Eng. 2021 Aug;49(8):1943-1972. doi: 10.1007/s10439-020-02704-9. Epub 2021 Jan 5. Ann Biomed Eng. 2021. PMID: 33403451 Review.
-
Biobanked Glioblastoma Patient-Derived Organoids as a Precision Medicine Model to Study Inhibition of Invasion.Int J Mol Sci. 2021 Oct 3;22(19):10720. doi: 10.3390/ijms221910720. Int J Mol Sci. 2021. PMID: 34639060 Free PMC article.
-
Rapid identification and validation of novel targeted approaches for Glioblastoma: A combined ex vivo-in vivo pharmaco-omic model.Exp Neurol. 2018 Jan;299(Pt B):281-288. doi: 10.1016/j.expneurol.2017.09.006. Epub 2017 Sep 18. Exp Neurol. 2018. PMID: 28923369 Review.
-
In vitro biomimetic models for glioblastoma-a promising tool for drug response studies.Drug Resist Updat. 2021 Mar;55:100753. doi: 10.1016/j.drup.2021.100753. Epub 2021 Feb 20. Drug Resist Updat. 2021. PMID: 33667959 Review.
-
Tumor Organoid as a Drug Screening Platform for Cancer Research.Curr Stem Cell Res Ther. 2024;19(9):1210-1250. doi: 10.2174/011574888X268366230922080423. Curr Stem Cell Res Ther. 2024. PMID: 37855289 Review.
Cited by
-
Fluidic Programmable Gravi-maze Array for High Throughput Multiorgan Drug Testing.bioRxiv [Preprint]. 2025 Jun 24:2025.06.18.660241. doi: 10.1101/2025.06.18.660241. bioRxiv. 2025. PMID: 40666863 Free PMC article. Preprint.
References
-
- Tamimi AF, Juweid M. Epidemiology and Outcome of Glioblastoma. In: De Vleeschouwer S, editor. Glioblastoma. Brisbane (AU) 2017. - PubMed
-
- Ellor SV, Pagano-Young TA, Avgeropoulos NG. Glioblastoma: background, standard treatment paradigms, and supportive care considerations. J Law Med Ethics. 2014;42(2):171–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
