

Prospective clinical study of sentinel node detection in bladder cancer using a hybrid tracer - Towards replacement of pelvic lymph node dissection in cases with sentinel node visualization on SPECT/CT?
- PMID: 40183956
- PMCID: PMC12316797
- DOI: 10.1007/s00259-025-07240-z
Prospective clinical study of sentinel node detection in bladder cancer using a hybrid tracer - Towards replacement of pelvic lymph node dissection in cases with sentinel node visualization on SPECT/CT?
Abstract
Purpose: Nodal staging in patients with muscle invasive bladder cancer (MIBC) or very high risk non-muscle invasive bladder cancer (vhNMIBC) aids to predict survival. The sentinel node (SN) procedure holds the promise to identify the diagnostically relevant first tumor-draining nodes while limiting the complication rate associate with a pelvic lymph node dissection (PLND), still considered the gold standard of nodal staging. Following an initial technical feasibility study, we prospectively evaluated the clinical impact of using peri-tumoral injections with the hybrid tracer indocyanine green (ICG)-99mTc-nanocolloid for SN procedures in bladder cancer.
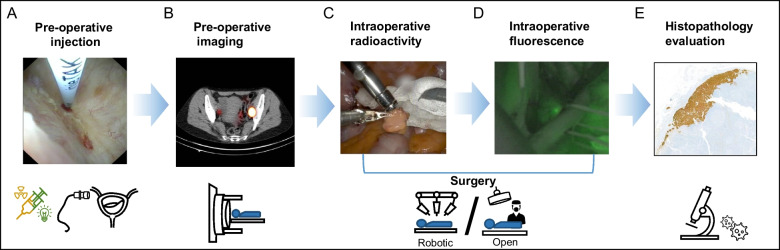
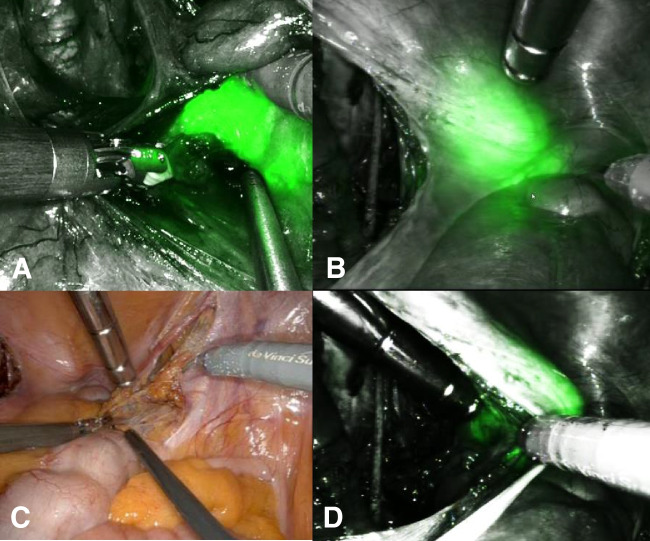
Methods: A total of 30 patients with vhNMIBC or MIBC, cN0M0 (with or without neo-adjuvant systemic therapy) scheduled for radical cystectomy with pelvic lymph node dissection (PLND) were enrolled in a prospective study. Patients received four to six transurethral peritumoral injections of ICG-99mTc-nanocolloid into the bladder for SN tracing. Preoperative lymphoscintigraphy and Single Photon Emission Computed Tomography (SPECT)/CT was performed the day before surgery. The intraoperative detection of SNs was supported by both fluorescence (utilizing a hand-held camera or fluorescence laparoscope) and radio-guidance (using hand-held, laparoscopic or DROP-IN probe tracing). Resected specimens, comprising both SNs and PLND tissue, were analyzed by the pathologist. Complications related to the tracer injection were documented and cancer-specific survival (CSS) and overall survival (OS) were studied using Kaplan-Meier survival curves.
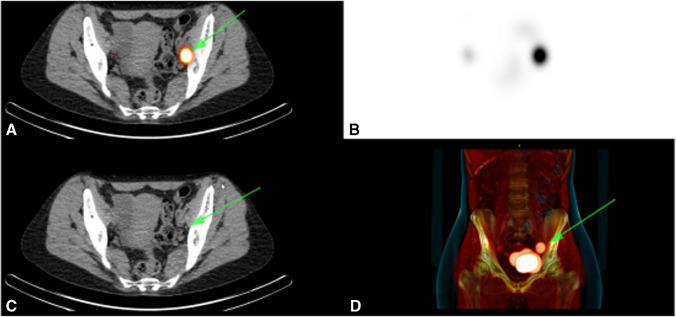
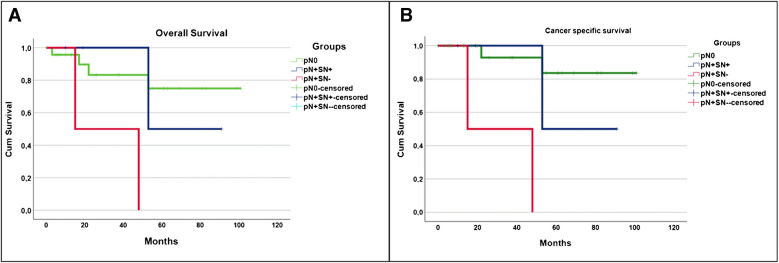
Results: SPECT/CT imaging revealed 31 SNs in 19 patients with non-visualization of SN in 11 patients (36.7%). During surgery, 4 additional SNs were identified based on fluorescent signals in 3 patients. In 1 patient who underwent open cystectomy, ex vivo evaluation of the PLND-specimen revealed an additional radioactive SN. The PLND yielded 592 lymph nodes (LNs; median 17 LNs/patient). In 5 out of 35 SNs (14.2%; no additional tumor positive LN in complementary PLND) and 3 out of 592 LNs (0.5%; 2 patients with non-visualization of SN) were identified as tumor-positive upon pathological evaluation. At mean follow up of 82 months (SD ± 7.1 months) 17% of patients died of disease. The 2 patients with non-visualization of SN and nodal metastases (0%) did worse than SN positive patients (75%). Of the 24 patients classified as pN0 8% died.
Conclusions: Preoperative SN-visualization on SPECT/CT was achieved in the majority of patients. Patients with SN non-visualization had an increased risk of nodal metastases and poorer outcome. In patients with metastases in the SN no additional nodal metastases were found in the complementary PLND.
Keywords: Bladder cancer; Fluorescence; Radio-guided surgery; Robotic surgery; Sentinel lymph node.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of NKI-AvL 2014, M14HSN study protocol. Consent to participate: Informed consent was obtained from all individual participants included in the study. Consent to publish: The authors affirm that human research participants provided informed consent for publication of the images in Figs. 1, 3 and 4 Competing interests: The authors have no relevant financial or non-financial interests to disclose.
Figures

References
-
- Witjes JA, Bruins HM, Carrión A, Cathomas R, Compérat EM, Efstathiou JA, et al. Muscle-invasive and metastatic bladder cancer. EAU Guidelines on muscle-invasive and metastatic bladder cancer. 2024.
-
- Perera M, McGrath S, Sengupta S, Crozier J, Bolton D, Lawrentschuk N. Pelvic lymph node dissection during radical cystectomy for muscle-invasive bladder cancer. Nat Rev Urol. 2018;15:686–92. - PubMed
-
- Bruins HM, Veskimae E, Hernandez V, Imamura M, Neuberger MM, Dahm P, et al. The impact of the extent of lymphadenectomy on oncologic outcomes in patients undergoing radical cystectomy for bladder cancer: a systematic review. Eur Urol. 2014;66:1065–77. - PubMed
-
- Horenblas S, Jansen L, Meinhardt W, Hoefnagel CA, de Jong D, Nieweg OE. Detection of occult metastasis in squamous cell carcinoma of the penis using a dynamic sentinel node procedure. J Urol. 2000;163:100–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
