

Comprehensive treatment strategy for pancreaticopleural fistula: A rare case report and review of 91 cases
- PMID: 40184110
- PMCID: PMC11709174
- DOI: 10.1097/MD.0000000000041184
Comprehensive treatment strategy for pancreaticopleural fistula: A rare case report and review of 91 cases
Abstract
Rationale: Pancreaticopleural fistula (PPF) is a rare but serious complication of pancreatic disease, typically resulting from the rupture of a pancreatic pseudocyst or ductal injury. The condition often leads to misdiagnosis due to its nonspecific clinical manifestations, including dyspnea and chest pain.
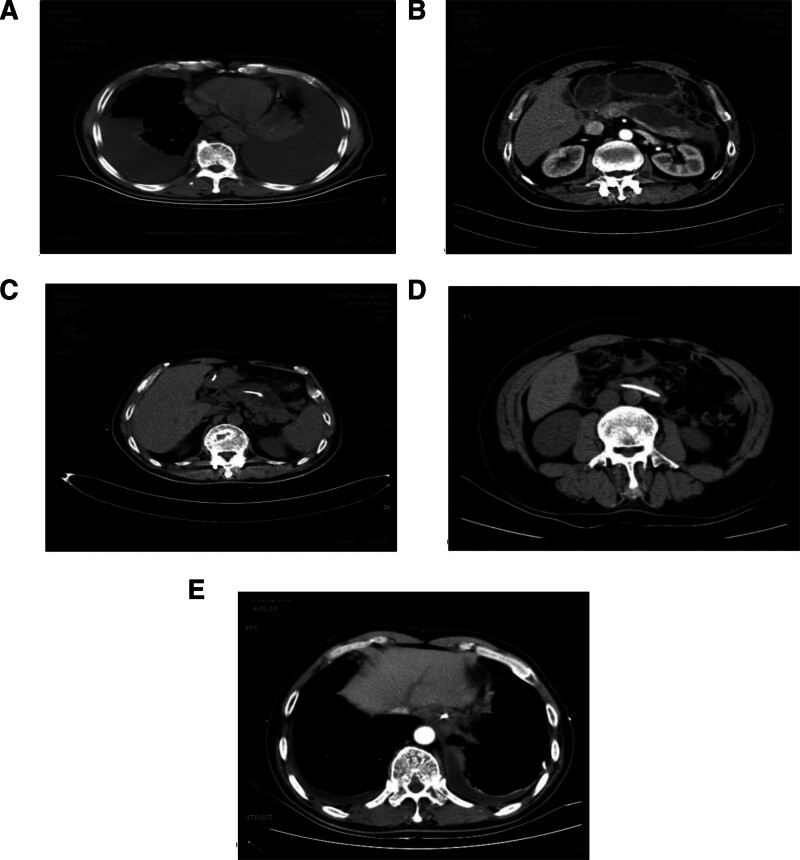
Patient concerns: A 61-year-old male with a history of alcohol and tobacco use presented with severe dyspnea, chest pain, and cough. He had been diagnosed with acute pancreatitis 9 months prior and intermittently experienced upper abdominal pain and distension post-treatment.
Diagnoses: PPF.
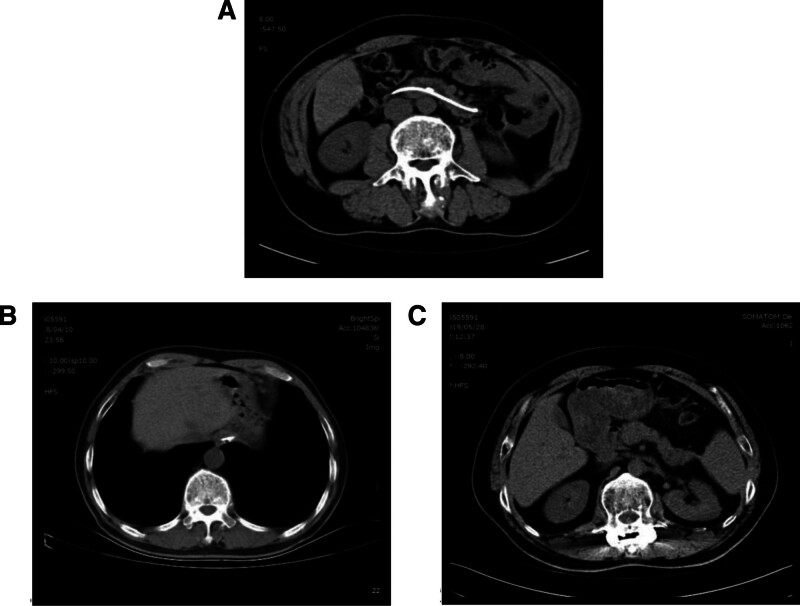
Interventions: The patient underwent thoracic drainage, nasopancreatic duct drainage, and pancreatic duct stent placement, along with parenteral nutrition and somatostatin therapy.
Outcomes: Treatment resulted in resolution of pleural effusion and pseudocyst. The patient had no recurrence during a 5-year follow-up period.
Lessons: This case demonstrates the effectiveness of a comprehensive treatment strategy combining thoracic and pancreatic drainage for PPF. Long-term follow-up is crucial for monitoring recurrence and assessing treatment efficacy. Future research should focus on optimizing treatment plans, particularly regarding the best timing for intervention and improving long-term outcomes.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to diclose.
Figures
References
-
- Chawla G, Niwas R, Chauhan NK, Dutt N, Yadav T, Jain P. Pancreatic pleural effusion masquerading as right sided tubercular pleural effusion. Monaldi Arch Chest Dis. 2019;89:3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
