

Implementation of a national AI technology program on cardiovascular outcomes and the health system
- PMID: 40186078
- PMCID: PMC12176617
- DOI: 10.1038/s41591-025-03620-y
Implementation of a national AI technology program on cardiovascular outcomes and the health system
Abstract
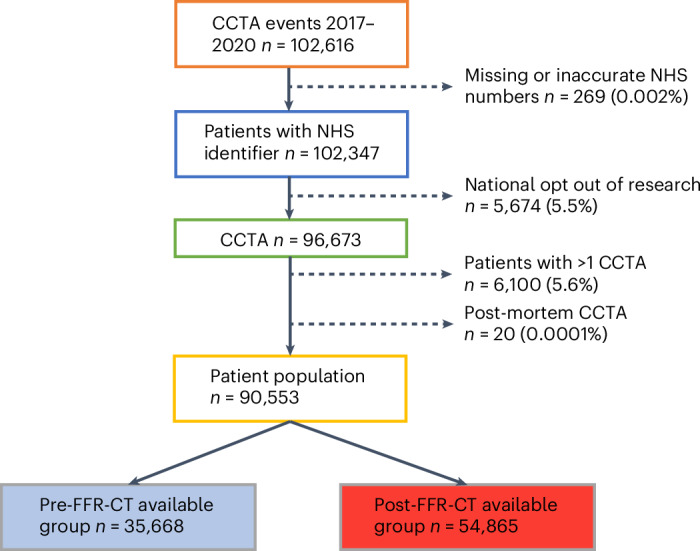
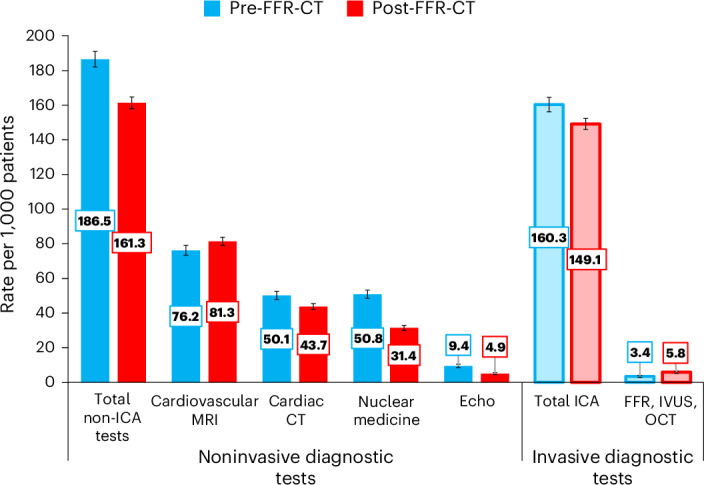
Coronary artery disease (CAD) is a major cause of ill health and death worldwide. Coronary computed tomographic angiography (CCTA) is the first-line investigation to detect CAD in symptomatic patients. This diagnostic approach risks greater second-line heart tests and treatments at a cost to the patient and health system. The National Health Service funded use of an artificial intelligence (AI) diagnostic tool, computed tomography (CT)-derived fractional flow reserve (FFR-CT), in patients with chest pain to improve physician decision-making and reduce downstream tests. This observational cohort study assessed the impact of FFR-CT on cardiovascular outcomes by including all patients investigated with CCTA during the national AI implementation program at 27 hospitals (CCTA n = 90,553 and FFR-CT n = 7,863). FFR-CT was safe, with no difference in all-cause (n = 1,134 (3.2%) versus 1,612 (2.9%), adjusted-hazard ratio (aHR) 1.00 (0.93-1.08), P = 0.97) or cardiovascular mortality (n = 465 (1.3%) versus 617 (1.1%), aHR 0.96 (0.85-1.08), P = 0.48), while reducing invasive coronary angiograms (n = 5,720 (16%) versus 8,183 (14.9%), aHR 0.93 (0.90-0.97), P < 0.001) and noninvasive cardiac tests (189/1,000 patients versus 167/1,000), P < 0.001). Implementation of an AI-diagnostic tool as part of a health intervention program was safe and beneficial to the patient pathway and health system with fewer cardiac tests at 2 years.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors received no specific funding for this work. S.M. and C.R. are employees of HeartFlow. An MRC Industrial Collaboration Agreement was signed between collaborators and HeartFlow. HeartFlow provided the pseudo-anonymized FFR-CT data but had no role in the study design, data collection, analysis, interpretation of the data, writing or decision to submit the manuscript. The other authors declare no competing interests.
Figures









References
-
- Gulati, M. et al. AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation144, e368–e454 (2021). - PubMed
-
- Knuuti, J. et al. ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J.41, 407–477 (2020). - PubMed
-
- Chest Pain of Recent Onset: Assessment and Diagnosis. NICE Guidelines (NICE, 2010).
-
- Inohara, T. et al. Appropriateness ratings of percutaneous coronary intervention in Japan and its association with the trend of noninvasive testing. JACC Cardiovasc. Inter.7, 1000–1009 (2014). - PubMed
-
- HeartFlow FFRCT for Estimating Fractional Flow Reserve from Coronary CT Angiography (MTG32) (National Institute for Health and Care Excellence, 2017); https://www.nice.org.uk/guidance/mtg32/resources
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
