

Open-source deep-learning models for segmentation of normal structures for prostatic and gynecological high-dose-rate brachytherapy: Comparison of architectures
- PMID: 40186596
- PMCID: PMC12148797
- DOI: 10.1002/acm2.70089
Open-source deep-learning models for segmentation of normal structures for prostatic and gynecological high-dose-rate brachytherapy: Comparison of architectures
Abstract
Background: The use of deep learning-based auto-contouring algorithms in various treatment planning services is increasingly common. There is a notable deficit of commercially or publicly available models trained on large or diverse datasets containing high-dose-rate (HDR) brachytherapy treatment scans, leading to poor performance on images that include HDR implants.
Purpose: To implement and evaluate automatic organs-at-risk (OARs) segmentation models for use in prostatic-and-gynecological computed tomography (CT)-guided high-dose-rate brachytherapy treatment planning.
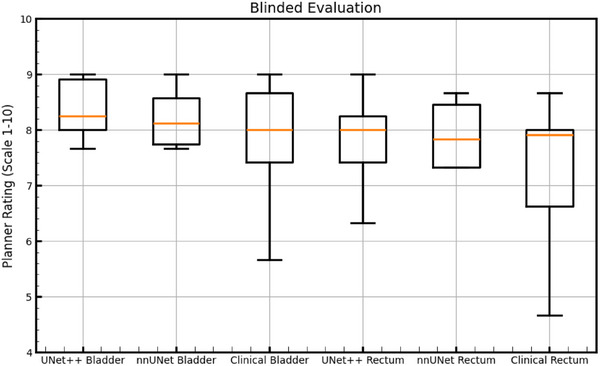
Methods and materials: 1316 computed tomography (CT) scans and corresponding segmentation files from 1105 prostatic-or-gynecological HDR patients treated at our institution from 2017 to 2024 were used for model training. Data sources comprised six CT scanners including a mobile CT unit with previously reported susceptibility to image streaking artifacts. Two UNet-derived model architectures, UNet++ and nnU-Net, were investigated for bladder and rectum model training. The models were tested on 100 CT scans and clinically-used segmentation files from 62 prostatic-or-gynecological HDR brachytherapy patients, disjoint from the training set, collected in 2024. Performance was evaluated using the Dice-Similarity-Coefficient (DSC) between model predicted contours and clinically-used contours on slices in common with the Clinical-Target-Volume (CTV). Additionally, a blinded evaluation of ten random test cases was conducted by three experienced planners.
Results: Median (interquartile range) 3D DSC on CTV-containing slices were 0.95 (0.04) and 0.87 (0.09) for the UNet++ bladder and rectum models, respectively, and 0.96 (0.03) and 0.88 (0.10) for the nnU-Net. The rank-sum test did not reveal statistically significant differences in these DSC (p = 0.15 and 0.27, respectively). The blinded evaluation scored trained models higher than clinically-used contours.
Conclusion: Both UNet-derived architectures perform similarly on the bladder and rectum and are adequately accurate to reduce contouring time in a review-and-edit context during HDR brachytherapy planning. The UNet++ models were chosen for implementation at our institution due to lower computing hardware requirements and are in routine clinical use.
Keywords: Auto‐contouring; brachytherapy; dice‐similarity‐coefficient; segmentation.
© 2025 The Author(s). Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
A novel network architecture for post-applicator placement CT auto-contouring in cervical cancer HDR brachytherapy.Med Phys. 2025 Jul;52(7):e17908. doi: 10.1002/mp.17908. Epub 2025 May 25. Med Phys. 2025. PMID: 40414687
-
Self-configuring nnU-Net for automatic delineation of the organs at risk and target in high-dose rate cervical brachytherapy, a low/middle-income country's experience.J Appl Clin Med Phys. 2023 Aug;24(8):e13988. doi: 10.1002/acm2.13988. Epub 2023 Apr 12. J Appl Clin Med Phys. 2023. PMID: 37042449 Free PMC article.
-
Dual convolution-transformer UNet (DCT-UNet) for organs at risk and clinical target volume segmentation in MRI for cervical cancer brachytherapy.Phys Med Biol. 2024 Oct 18;69(21). doi: 10.1088/1361-6560/ad84b2. Phys Med Biol. 2024. PMID: 39378904
-
Use of three-dimensional radiation therapy planning tools and intraoperative ultrasound to evaluate high dose rate prostate brachytherapy implants.Int J Radiat Oncol Biol Phys. 1999 Feb 1;43(3):571-8. doi: 10.1016/s0360-3016(98)00420-9. Int J Radiat Oncol Biol Phys. 1999. PMID: 10078639 Review.
-
A review of artificial intelligence in brachytherapy.J Appl Clin Med Phys. 2025 Jun;26(6):e70034. doi: 10.1002/acm2.70034. Epub 2025 Feb 27. J Appl Clin Med Phys. 2025. PMID: 40014044 Free PMC article. Review.
References
-
- Hoque SMH, Pirrone G, Matrone F, et al. Clinical use of a commercial artificial intelligence‐based software for autocontouring in radiation therapy: geometric performance and dosimetric impact. Cancers (Basel). 2023;15(24):5735. doi: 10.3390/cancers15245735. Published 2023 Dec 7. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
