

Colorectal cancer incidence after the first surveillance colonoscopy and the need for ongoing surveillance: a retrospective, cohort analysis
- PMID: 40187891
- PMCID: PMC12418537
- DOI: 10.1136/gutjnl-2024-334242
Colorectal cancer incidence after the first surveillance colonoscopy and the need for ongoing surveillance: a retrospective, cohort analysis
Abstract
Background: Recommendations for the first postpolypectomy surveillance colonoscopy (SC1), based on stratifying postpolypectomy colorectal cancer (CRC) risk, are well established. Limited data inform recommendations for surveillance beyond SC1.
Objective: We investigated which patient groups need surveillance beyond SC1.
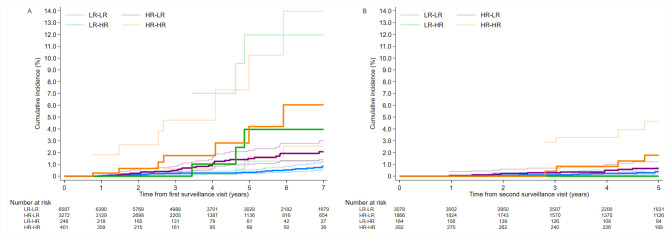
Design: Retrospective analysis of patients who underwent colonoscopy with polypectomy at 17 UK hospitals, mostly from 2000 to 2010, and had ≥1 surveillance colonoscopies. Cancer and death data were collected through 2017. We examined patients in groups defined by risk at baseline and SC1, applying risk definitions from the 2020 UK postpolypectomy surveillance guidelines: 'low risk, low risk' (LR-LR), 'high risk, low risk' (HR-LR), 'low risk, high risk' (LR-HR) and 'high risk, high risk' (HR-HR). We examined CRC incidence after SC1, censoring at any second surveillance colonoscopy (SC2), and after SC2 through end of follow-up. We compared incidence with general population incidence using standardised incidence ratios (SIRs).
Results: Analyses included 10 508 patients: LR-LR=6587 (63%), HR-LR=3272 (31%), LR-HR=248 (2%) and HR-HR=401 (4%). Median follow-up from SC1 was 8.0 years and 151 CRCs were diagnosed. Compared with the general population, CRC incidence after SC1 was lower in the LR-LR group (SIR 0.48, 95% CI 0.34 to 0.67), non-significantly different in the HR-LR (SIR 1.17, 0.85 to 1.58) or LR-HR (SIR 2.51, 0.81 to 5.85) groups, but higher in the HR-HR group (SIR 2.84, 1.30 to 5.39). After SC2, CRC incidence in the HR-HR group was no longer higher than in the general population (SIR 1.86, 0.89 to 3.42).
Conclusion: Patients with high-risk findings at both baseline and SC1 needed an SC2, while those with low-risk findings at SC1 did not, regardless of their baseline findings.
Keywords: COLORECTAL CANCER; POLYP; SURVEILLANCE.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: AJC, as Chief Investigator, was the recipient of all the funding. All other authors declare no competing interests.
Figures


References
-
- Rutter MD, East J, Rees CJ, et al. British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland/Public Health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut. 2020;69:201–23. doi: 10.1136/gutjnl-2019-319858. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous