

Effect of ICU Quality Control and Secondary Analysis: A 12-Year Multicenter Quality Improvement Project
- PMID: 40191175
- PMCID: PMC11972604
- DOI: 10.2147/JMDH.S509567
Effect of ICU Quality Control and Secondary Analysis: A 12-Year Multicenter Quality Improvement Project
Abstract
Background: China's aging population and increasing demand for critical care pose significant challenges to ICU quality improvement (QI). This study evaluates the impact of a 12-year multicenter QI initiative on ICU performance and patient outcomes in the context of resource constraints.
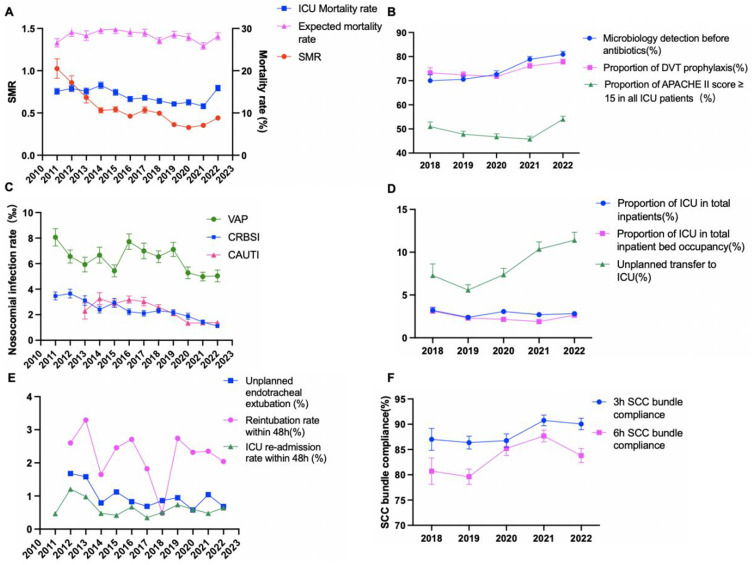
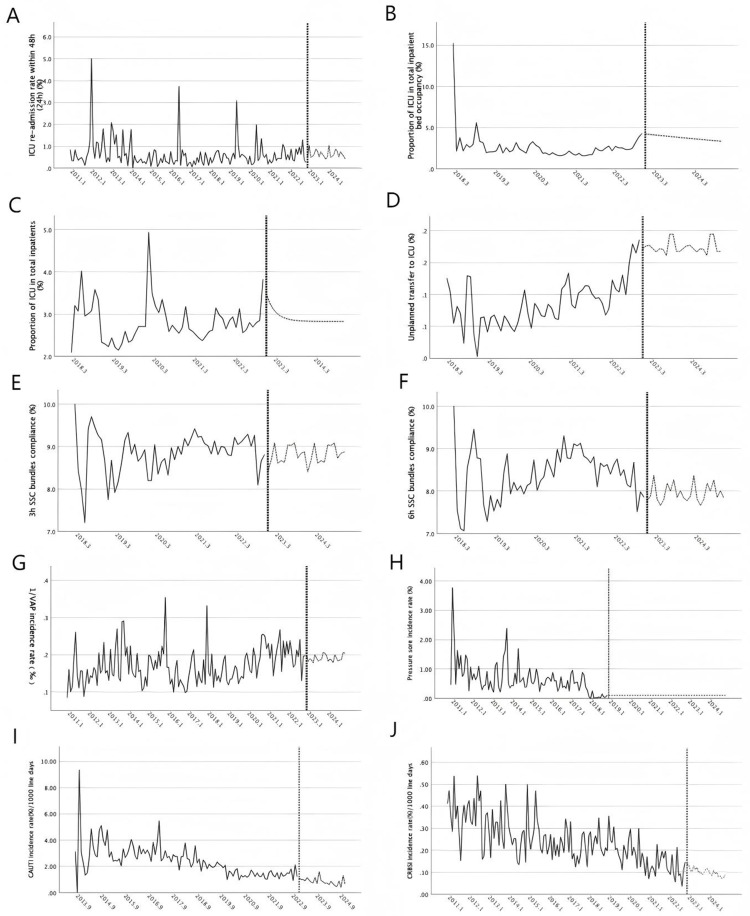
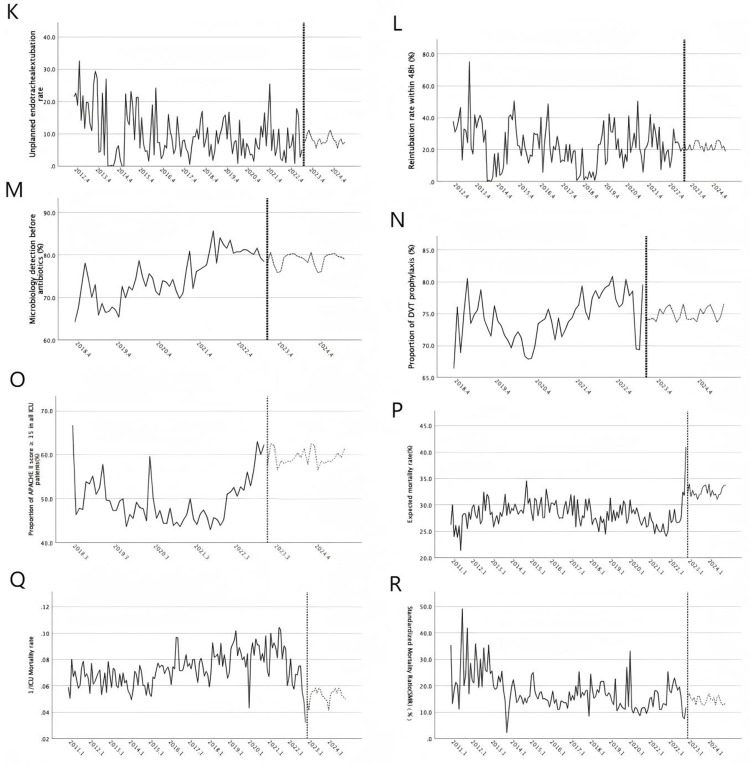
Methods: A pre-post intervention study was conducted across 75 ICUs in Beijing from January 2011 to December 2022. Key interventions included the establishment of QI teams, infection prevention protocols, pain and sedation management, nutritional support, and early mobilization strategies based on the PDCA cycle, as well as regular training and feedback. Primary outcomes included ICU mortality, standardized mortality ratio (SMR) (ratio of observed to expected deaths, adjusted for risk), and healthcare-associated infections (HAIs), such as VAP, CLABSI, and CAUTI rates. Secondary outcomes included unplanned extubation rates, reintubation within 48 hours, and ICU readmission rates within 48 hours.
Results: Analysis of 425,534 patient records from 5396 reports revealed significant improvements. The proportion of ICU admissions among total inpatients increased from 4.1% in 2011 to 7.3% in 2022 (P < 0.001), and the proportion of patients with APACHE II scores ≥15 rose from 52.0% to 67.5% (P < 0.001). Compliance with 3-hour and 6-hour sepsis bundles increased (P < 0.001), and microbiological testing before antibiotic administration also improved (P < 0.001). Outcome indicators showed significant reductions in CRBSI and CAUTI rates (P < 0.001), ICU mortality (P < 0.001), and SMR (P < 0.001). VAP rates decreased from 6.29 to below 5.0 per 1000 ventilator days. ICU readmission rates and unplanned transfers slightly increased but remained low (P > 0.05).
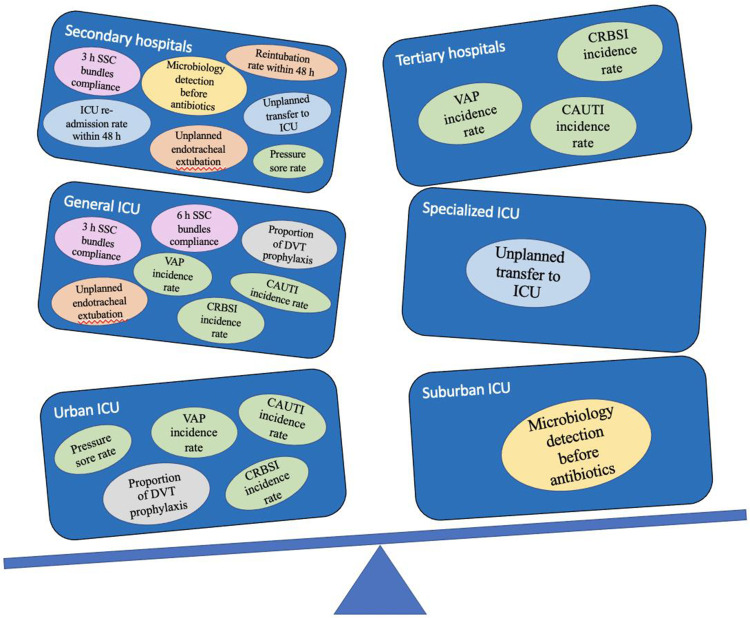
Conclusion: The study highlights the importance of addressing structural, process, and outcome indicators for effective ICU management. Continued monitoring and targeted interventions for high-risk ICUs are essential to sustaining quality improvements.
Keywords: data analysis; intensive care unit; mortality rate; patient prognosis; quality improvement.
© 2025 Qiu et al.
Conflict of interest statement
The authors declared that they have no conflicts of interest regarding this work.
Figures
Similar articles
-
Quality metrics and outcomes among critically ill patients in China: results of the national clinical quality control indicators for critical care medicine survey 2015-2019.Chin Med J (Engl). 2022 May 5;135(9):1064-1075. doi: 10.1097/CM9.0000000000001933. Chin Med J (Engl). 2022. PMID: 35773965 Free PMC article.
-
Evaluation of ICUs and weight of quality control indicators: an exploratory study based on Chinese ICU quality data from 2015 to 2020.Front Med. 2023 Aug;17(4):675-684. doi: 10.1007/s11684-022-0970-x. Epub 2023 Apr 15. Front Med. 2023. PMID: 37060524 Free PMC article.
-
Comparative Study Between Medical/Surgical Intensive Care Units vs. Mixed Intensive Care Units in Key Performance Indicators.Cureus. 2024 Nov 20;16(11):e74100. doi: 10.7759/cureus.74100. eCollection 2024 Nov. Cureus. 2024. PMID: 39712857 Free PMC article.
-
A Quality Improvement Project to Decrease CLABSIs in Non-ICU Settings.Qual Manag Health Care. 2023 Jul-Sep 01;32(3):189-196. doi: 10.1097/QMH.0000000000000375. Epub 2022 Nov 5. Qual Manag Health Care. 2023. PMID: 36346987 Review.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
References
LinkOut - more resources
Full Text Sources
