

Correlation of Liver Fibrosis using Noninvasive Transient Elastography with Histological Staging in Infants with Cholestasis - A Prospective Analytical Study
- PMID: 40191482
- PMCID: PMC11968036
- DOI: 10.4103/jiaps.jiaps_138_24
Correlation of Liver Fibrosis using Noninvasive Transient Elastography with Histological Staging in Infants with Cholestasis - A Prospective Analytical Study
Abstract
Aims: This study primarily aimed to correlate liver fibrosis (LF) assessed by transient elastography (TE) using liver stiffness measurement (LSM score) with liver biopsy fibrosis scoring (METAVIR score) in biliary atresia (BA). Secondary objectives were to assess the diagnostic accuracy of TE in distinguishing BA from other causes of neonatal cholestasis (NC) and the correlation of preoperative LSM score with surgical outcomes 3 months post Kasai portoenterostomy.
Methodology: Infants under 6 months with conjugated hyperbilirubinemia (July 2022-February 2024) were cases and age- and gender-matched healthy infants served as controls. Cases were evaluated using predefined standard diagnostic tests and TE using Fibroscan® Expert 630 (Echosens) device was additionally performed preoperatively and 3 months postoperatively. METAVIR scoring was calculated on liver histopathology.
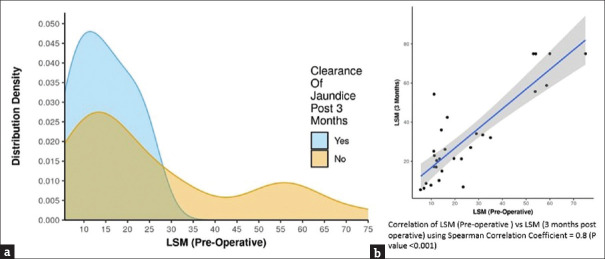
Results: Fifty-one NC patients (28 boys, 23 girls) were included. A preoperative LSM ≥ 11.4 predicted significant fibrosis (METAVIR score - F3/F4) with 94% sensitivity and 46% specificity (P = 0.053). A preoperative LSM ≥ 13.2 fairly predicted the presence of BA with 74% sensitivity, 71% specificity (P = 0.006), and 72.5% diagnostic accuracy. Median preoperative LSM (interquartile range) for clearance of jaundice (COJ) (14.1 [10.28-18.48]) versus no clearance (15.7 [12.1-35]) showed no statistical difference (P = 0.359).
Discussion and conclusion: TE is an effective noninvasive screening tool to differentiate BA from other causes of NC with a cutoff of >13.2 kPa. The predictive value of TE for postoperative COJ and complications like cholangitis based on the preoperative LF measurements cannot be commented on based on our results.
Keywords: Biliary atresia; METAVIR score; liver biopsy; liver fibrosis; neonatal cholestasis; transient elastography; ultrasound shear wave elastography.
Copyright: © 2025 Journal of Indian Association of Pediatric Surgeons.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Sanchez-Valle A, Kassira N, Varela VC, Radu SC, Paidas C, Kirby RS. Biliary atresia:epidemiology, genetics, clinical update, and public health perspective. Adv Pediatr. 2017;64:285–305. - PubMed
-
- Kim JR, Hwang JY, Yoon HM, Jung AY, Lee JS, Kim JS, et al. Risk estimation for biliary atresia in patients with neonatal cholestasis: Development and validation of a risk score. Radiology. 2018;288:262–9. - PubMed
-
- Hartley JL, Davenport M, Kelly DA. Biliary atresia. Lancet. 2009;374:1704–13. - PubMed
-
- Wang Y, Jia LQ, Hu YX, Xin Y, Yang X, Wang XM. Development and validation of a nomogram incorporating ultrasonic and elastic findings for the preoperative diagnosis of biliary atresia. Acad Radiol. 2021;28(Suppl 1):S55–63. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous