

High-Precision Identification of Sensory and Motor Branches of the Recurrent Laryngeal Nerve Via Autofluorescence System in Thyroid Surgery
- PMID: 40196105
- PMCID: PMC11975449
- DOI: 10.7759/cureus.80262
High-Precision Identification of Sensory and Motor Branches of the Recurrent Laryngeal Nerve Via Autofluorescence System in Thyroid Surgery
Abstract
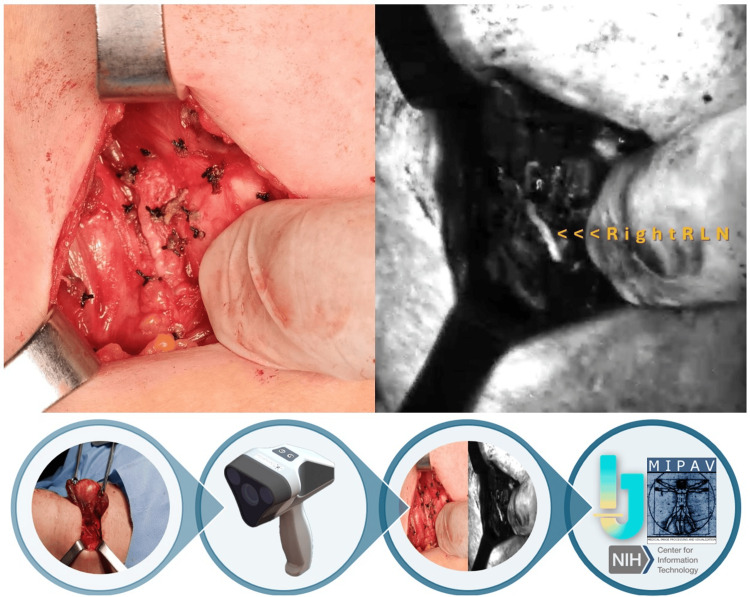
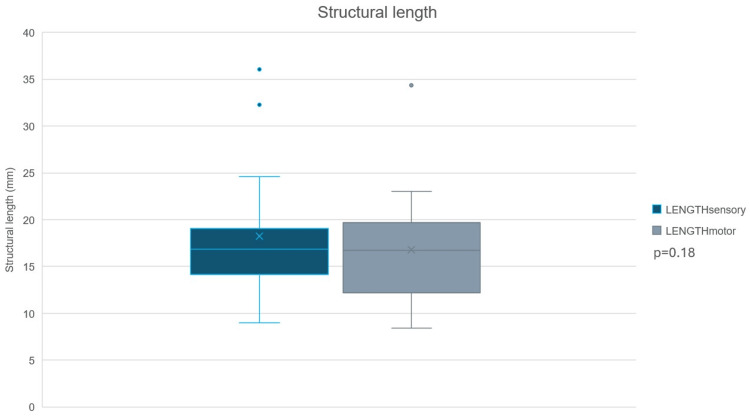
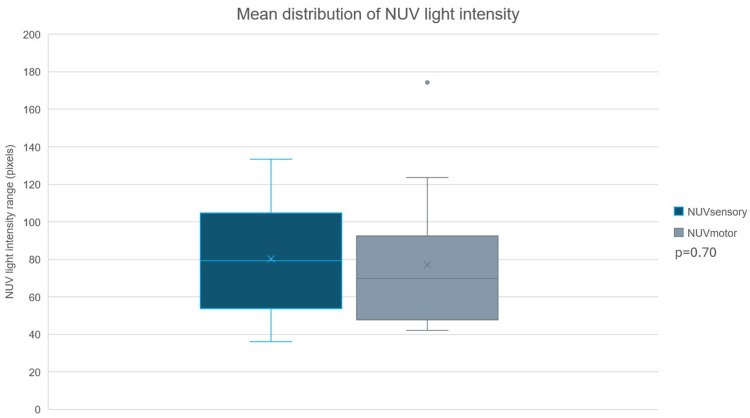
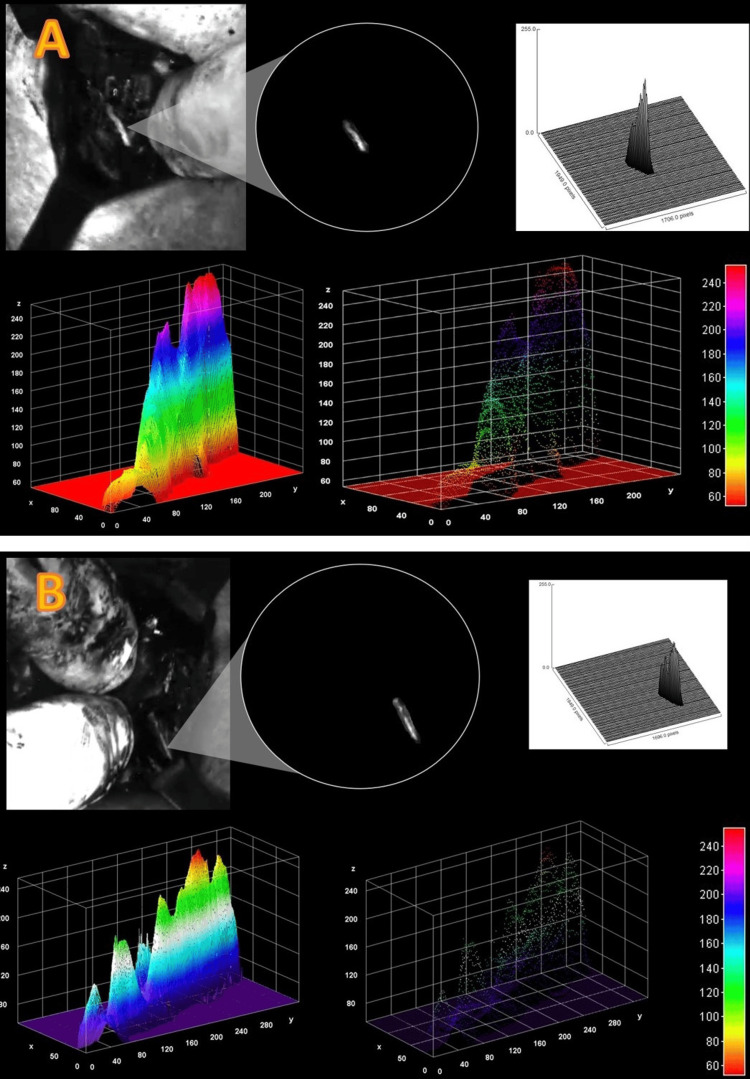
Recurrent laryngeal nerve (RLN) injury is a critical complication in thyroidectomy, with the severe sequelae of operation-related vocal cord palsies. The primary therapy following RLN injury includes voice therapy and surgical reintervention, both of which render subpar results paired with a long road to recovery. Despite the development of technical measures to prevent inadvertent operational injury of the RLN, its occurrence is still a concern. A newly developed handheld device with nerve autofluorescence technology has emerged as a visual aid tool for the intraoperative identification of nervous anatomical landmarks in thyroid surgery, showcasing promising initial findings. This study evaluates the efficacy of the aforementioned device in the intraoperative identification and differentiation of sensory and motor branches of the RLN. Sixteen patients undergoing thyroid surgery were included in this study, of which 16 RLNs and its branches were examined. Basic demographics, indication for thyroid surgery, and postoperative outcomes were identified. Multiple intraoperative images were analyzed through image processing software programs for the total number of nerves and branches, type of branch (e.g., sensory versus motor branches), near-ultraviolet (NUV) light intensity emitted by the nerve structures, and length and angular aperture of branches. The ability to prevent operation-related RLN injury was clinically evaluated at postoperative follow-up. Following analyses, no significant difference was observed between NUV light intensity (p=0.70) or structural length (p=0.18) between sensory and motor nerve branches of the RLN. This was further confirmed by fast Fourier transform (FFT) analyses and three-dimensional surface plots. No partial or total vocal cord palsies were recorded in the perioperative period, thus confirming the accuracy for intraoperative identification of the RLN and the preservation of structural integrity irrespective of surgical technique or type of branch (sensory or motor). Altogether, these findings highlight the potential of autofluorescence technology to enhance surgical precision, improve nerve preservation, and reduce the risk of nerve injury via safe surgical navigation in comparison to current intraoperative neuromonitoring systems limited to motor branch detection.
Keywords: autofluorescence; navigational surgery; optical imaging; surgical enhancement; thyroidectomy.
Copyright © 2025, Dip et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: Fernando Dip, Rene Aleman, Raul J. Rosenthal, and Alberto Rancati. declare(s) non-financial support from Dendrite® Imaging Inc. Investment and development. . Fernando Dip, Rene Aleman, Raul J. Rosenthal, Alaberto Rancati. declare(s) non-financial support from Intelligent Surgical Eye®. Investment and development. . Intellectual property info: The nerve autofluorescence optic imaging technology in the Dendrite® device is proprietary to Dendrite® Imaging Inc (Gera, Germany). All images are property of the authors associated to the aforementioned company. The present manuscript has resulted in no compensation to the authors and/or disclosed companies. Other relationships: Dr. Dip, Dr. Rosenthal, Dr. Rancati, and Dr. Aleman are active developing and investing members for Dendrite® Imaging Inc (Gera, Germany).
Figures
Similar articles
-
Anatomical, Functional, and Dynamic Evidences Obtained by Intraoperative Neuromonitoring Improving the Standards of Thyroidectomy.Sisli Etfal Hastan Tip Bul. 2021 Jul 2;55(2):146-155. doi: 10.14744/SEMB.2021.45548. eCollection 2021. Sisli Etfal Hastan Tip Bul. 2021. PMID: 34349588 Free PMC article. Review.
-
Enhancing Recurrent Laryngeal Nerve Detection with Neural Autofluorescence in Thyroid Surgery.J Am Coll Surg. 2025 Jul 31. doi: 10.1097/XCS.0000000000001540. Online ahead of print. J Am Coll Surg. 2025. PMID: 40742189
-
A Review of Methods for the Preservation of Laryngeal Nerves During Thyroidectomy.Sisli Etfal Hastan Tip Bul. 2018 Jun 18;52(2):79-91. doi: 10.14744/SEMB.2018.37928. eCollection 2018. Sisli Etfal Hastan Tip Bul. 2018. PMID: 32595378 Free PMC article. Review.
-
Varied Recurrent Laryngeal Nerve Course Is Associated with Increased Risk of Nerve Dysfunction During Thyroidectomy: Results of the Surgical Anatomy of the Recurrent Laryngeal Nerve in Thyroid Surgery Study, an International Multicenter Prospective Anatomic and Electrophysiologic Study of 1000 Monitored Nerves at Risk from the International Neural Monitoring Study Group.Thyroid. 2021 Nov;31(11):1730-1740. doi: 10.1089/thy.2021.0155. Thyroid. 2021. PMID: 34541890
-
Clinical value of intraoperative neuromonitoring of the recurrent laryngeal nerves in improving outcomes of surgery for well-differentiated thyroid cancer.Pol Przegl Chir. 2011 Apr;83(4):196-203. doi: 10.2478/v10035-011-0030-8. Pol Przegl Chir. 2011. PMID: 22166358
Cited by
-
The Sensory Gatekeeper of the Larynx: Anatomy and Clinical Importance of the Internal Branch of the Superior Laryngeal Nerve.Diagnostics (Basel). 2025 Jul 4;15(13):1711. doi: 10.3390/diagnostics15131711. Diagnostics (Basel). 2025. PMID: 40647708 Free PMC article. Review.
References
-
- Kenny BJ, Bordoni B. StatPearls [Internet] Treasure Island, FL: StatPearls Publishing; 2025. Neuroanatomy, cranial nerve 10 (vagus nerve)
-
- Relationship between vocal cord paralysis and benign thyroid disease. Collazo-Clavell ML, Gharib H, Maragos NE. Head Neck. 1995;17:24–30. - PubMed
-
- Recurrent nerve injury after total thyroidectomy: risk factor analysis of a targeted NSQIP data set. Mahvi DA, Saadat LV, Knell J, Urman RD, Whang EE, Cho NL. Am Surg. 2023;89:1396–1404. - PubMed
-
- Recurrent laryngeal nerve paralysis following thyroidectomy: analysis of factors affecting nerve recovery. Mohammad R, Huh G, Cha W, Jeong WJ. Laryngoscope. 2022;132:1692–1696. - PubMed
LinkOut - more resources
Full Text Sources