

This is a preprint.
Reinfection with SARS-CoV-2 in the Omicron Era is Associated with Increased Risk of Post-Acute Sequelae of SARS-CoV-2 Infection: A RECOVER-EHR Cohort Study
- PMID: 40196285
- PMCID: PMC11974971
- DOI: 10.1101/2025.03.28.25324858
Reinfection with SARS-CoV-2 in the Omicron Era is Associated with Increased Risk of Post-Acute Sequelae of SARS-CoV-2 Infection: A RECOVER-EHR Cohort Study
Abstract
Importance: Post-acute sequelae of SARS-CoV-2 infection (PASC) remains a major public health challenge. While previous studies have focused on characterizing PASC and identifying its subphenotypes in children and adolescents following an initial SARS-CoV-2 infection, the risks of PASC with Omicron-variant reinfections remain unclear. Using a real-world data approach, this study investigates the risks of PASC following reinfections during the Omicron phase in the pediatric population.
Objective: To investigate the risks of PASC diagnosis and 24 PASC symptoms and conditions after reinfection of SARS-CoV-2 during Omicron period in the pediatric population.
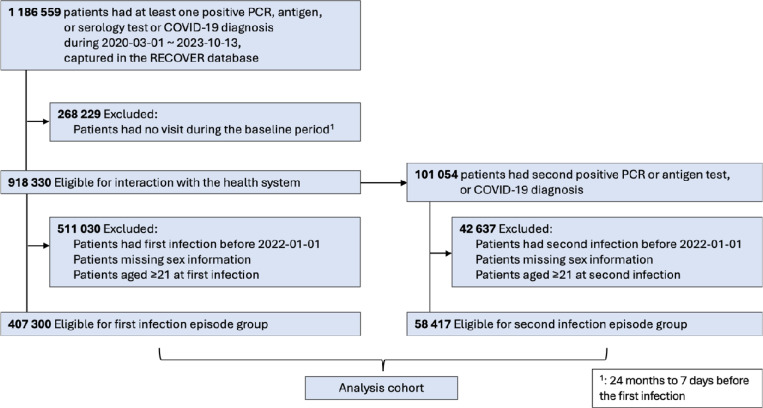
Design setting and participants: This retrospective cohort study used data from the RECOVER consortium comprising 40 children's hospitals and health institutions in U.S. between January 2022 and October 2023.
Exposures: A second SARS-CoV-2 infection, confirmed by a positive polymerase-chain-reaction (PCR) or antigen tests, or a diagnose of COVID-19, occurring at least 60 days after the initial infection, compared to the initial infection.
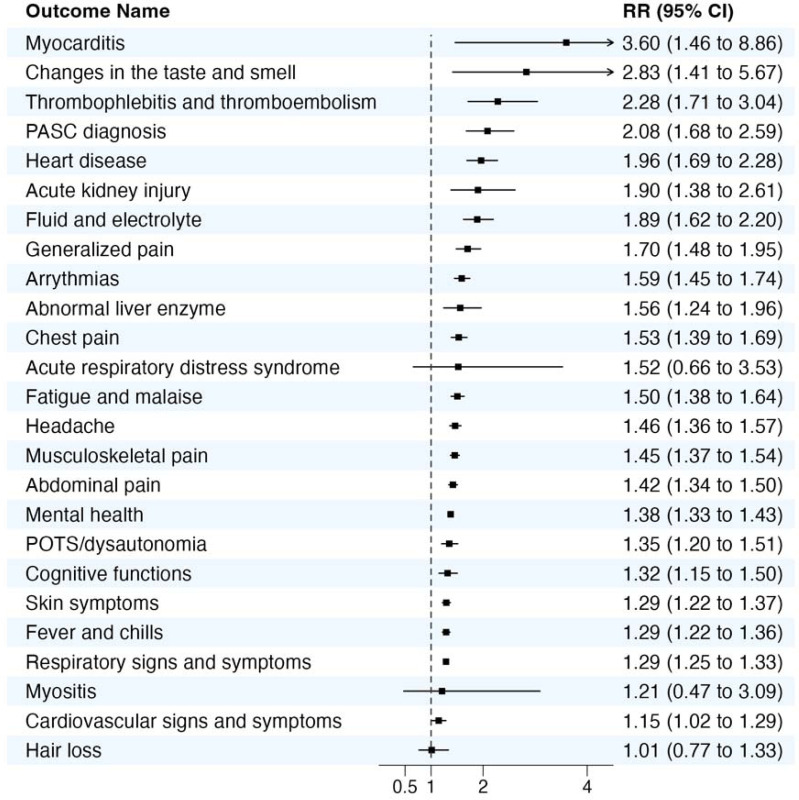
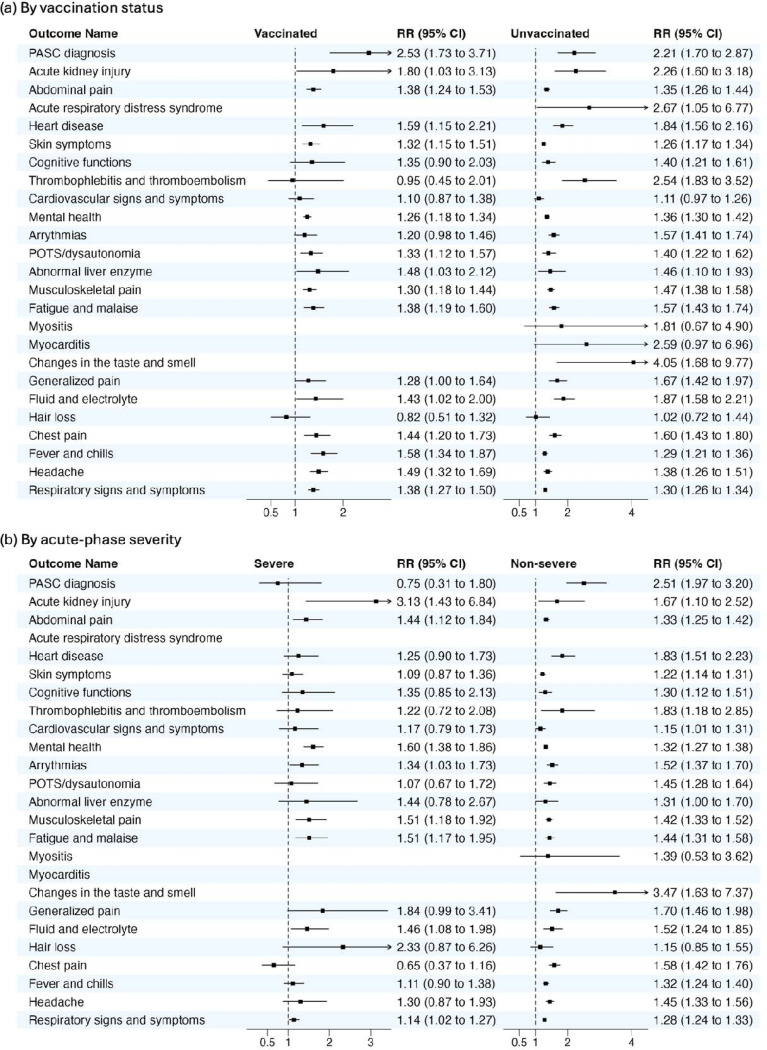
Main outcomes and measures: PASC was identified using two approaches: (1) the ICD-10-CM diagnosis code U09.9 and (2) a symptom-based definition including 24 physician-identified symptoms and conditions. Absolute risks of incident PASC were reported, and relative risks (RRs) were calculated by comparing the second infection episode with the first infection episode groups using a modified Poisson regression model, adjusting for demographic, clinical, and healthcare utilization factors through exact matching and propensity scoring matching.
Results: A total of 465,717 individuals under 21 years old (mean [SD] age 8.17 [6.58] years; 52% male) were included. Compared to the first infection, a second infection was associated with significantly increased risk of an overall PASC diagnosis (RR, 2.08; 95% confidence interval [CI], 1.68-2.59), and with many specific conditions including: myocarditis (RR, 3.60; 95% CI, 1.46-8.86); changes in taste and smell (RR, 2.83; 95% CI, 1.41-5.67); thrombophlebitis and thromboembolism (RR, 2.28; 95% CI, 1.71-3.04); heart disease (RR, 1.96; 95% CI, 1.69 to 2.28); acute kidney injury (RR, 1.90; 95% CI, 1.38 to 2.61); fluid and electrolyte (RR, 1.89; 95% CI, 1.62 to 2.20); generalized pain (RR, 1.70; 95% CI, 1.48 to ; arrhythmias (RR, 1.59; 95% CI, 1.45-1.74); abnormal liver enzyme (RR, 1.56; 95% CI, 1.24 to ; fatigue and malaise (RR, 1.50; 95% CI, 1.38 to 1.64); musculoskeletal pain (RR, 1.45; 95% CI, 1.37 to 1.54); abdominal pain (RR, 1.42; 95% CI, 1.34 to 1.50); postural orthostatic tachycardia syndromes (POTS)/dysautonomia (RR, 1.35; 95% CI, 1.20 to 1.51); cognitive functions (RR, 1.32; 95% CI, 1.15 to 1.50); and respiratory signs and symptoms (RR, 1.29; 95% CI, 1.25 to 1.33). The risks were consistent across various organ systems, including cardiovascular, respiratory, gastrointestinal, neurological, and musculoskeletal systems.
Conclusions and relevance: Children and adolescents face significantly higher risk of various PASC outcomes after reinfection with SARS-CoV-2. These findings suggest a cumulative risk of PASC and highlight the urgent need for targeted prevention strategies to reduce reinfections, which includes an increased emphasis on initial or re-vaccination of children.
Conflict of interest statement
Dr. Jhaveri is a consultant for AstraZeneca, Seqirus, Gilead, Sanofi; receives an editorial stipend from the Pediatric Infectious Diseases Society; research support from GSK; and royalties from Up To Date/Wolters Kluwer. All other co-authors have no conflicts of interest to report.
Figures
References
-
- National Institutes of Health (NIH). What is Long COVID? Building our understanding about recovery, https://recovercovid.org/long-covid (2024).
-
- Centers for Disease Control and Prevention (CDC). Long COVID or Post-COVID Conditions, https://www.cdc.gov/covid/long-term-effects/?CDC_AAref_Val=https://www.c... (2023).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous