

Prognosis of liver abscess in the intensive care unit (POLAIR), a multicentre observational study
- PMID: 40197508
- PMCID: PMC11974115
- DOI: 10.1186/s13054-025-05376-w
Prognosis of liver abscess in the intensive care unit (POLAIR), a multicentre observational study
Abstract
Background: Liver abscess (LA) is a rare but potentially serious condition with a high mortality rate. Current epidemiological data of LA patients requiring intensive care unit (ICU) admission are limited.
Methods: This multicentre retrospective study included adults admitted to 24 ICUs in France between January 2010 and December 2020. Risk factors for mortality were identified by multivariate analysis. A propensity score was used to adjust for confounders related to the presence of portal vein thrombosis.
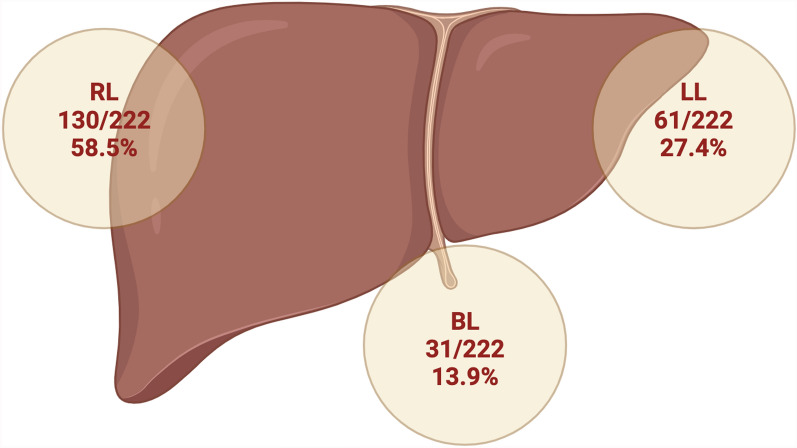
Results: 335 patients were enrolled. The median age was 66 years [53-73] and 68% were male. Commons comorbidities included diabetes (29.9%) and cancer or haematological disease. Septic shock was the main reason for admission (58%). The median SAPS2 score at ICU admission was 42 [31-53] and the SOFA score was 6 [3-9]. The putative origin of LA was biliary (31%), while 40% were cryptogenic. Most patients (60%) had a solitary LA, involving the right lobe (38.8%), with a median diameter of 67 mm [47-91]. Associated portal vein thrombosis (PVT) was present in 13.4% of cases. Microbiological documentation was obtained in 82% of patients, showing gram-negative bacilli (59.7%), mainly Escherichia coli (19.6%) and Klebsiella spp. (19.1%), and gram-positive cocci (29.6%), mainly Streptococcus spp. (17.1%). Drainage was performed in 62% of cases, 40% within 48 h. The median duration of antibiotic therapy was 35 days [21-42]. During hospitalisation, 62% of patients required vasopressors and 29% required mechanical ventilation. In-ICU mortality was 11.6%. Multivariate analysis showed that organ dysfunction illustrated by SOFA score (HR 3.45 [1.95-6.09], p < 0.001) and PVT (HR 3.14 [1.54-6.39], p = 0.001) were significant risk factors for mortality. Drainage was not associated with improved short-term survival (HR 1.22 [0.65-2.72], p = 0.52). In the population matched for PVT confounders, a higher sofa score was the only factor associated with mortality (HR 3.11 [1.76-5.49] IC95%, p = 0.001).
Conclusions: This multicentre study illustrates the severity of LA in French intensive care units and identifies organ dysfunction (SOFA score) and portal vein thrombosis as major risk factors for mortality. Prospective studies are needed to improve management strategies, as the survival benefit of drainage is unclear.
Keywords: Intensive care; Liver abscess; Microbiology; Mortality; Portal vein thrombosis; Prognosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study received ethical approval from the Ethics Committee of the Société de Réanimation de Langue Française (SRLF): reference CE SRLF 21-87. The patient cohort was registered with the Commition Nationale de l’Information et des Libertés (CNIL) under the MR004 framework, registration number 2224428. The methodological quality of the study was assessed according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines (Additional file 3). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Rossi G, Nguyen Y, Lafont E, Rossi B, Canouï E, Roux O, et al. Large retrospective study analysing predictive factors of primary treatment failure, recurrence and death in pyogenic liver abscesses. Infection. 2022;50(5):1205–15. - PubMed
-
- Oliosi E, Rossi G, Nguyen Y, Honsel V, Bert F, Roux O, et al. Enterococcal pyogenic liver abscesses: high risk of treatment failure and mortality. Eur J Clin Microbiol Infect Dis. 2023;42(2):193–9. - PubMed
-
- Jepsen P, Vilstrup H, Schønheyder HC, Sørensen HT. A nationwide study of the incidence and 30-day mortality rate of pyogenic liver abscess in Denmark, 1977–2002. Aliment Pharmacol Ther. 2005;21(10):1185–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
